Antiparkinsonian Drugs
Pharmacotherapy of Parkinson's disease — levodopa, dopaminergic agents, anticholinergics, recent advances.
Past RGUHS + DNB + MPMSU + MUHS · 30
MPMSUJan '25
DNBApr '23
DNBOct '23
MUHSWinter '22
DNBDec '21
MUHSSummer '21
RGUHSNov '20
RGUHSJun '20
MPMSU2019
MPMSUMay '19
MUHSWinter '19
RGUHSNov '17
MPMSU2017
MUHSSummer '17 Suppl
RGUHSNov '16
MUHSSummer '16
DNBDec '14
RGUHSOct '10
MPMSU2010
MPMSU2010
RGUHSOct '09
RGUHSMay '09
RGUHSApr '08
RGUHSApr '07
MPMSU2006
MPMSU2005
MPMSU2005
MPMSU1998
MPMSU1995
MPMSU1992
Parkinson's Disease (Antiparkinsonian Drugs)
1. Definition & overview
- Parkinsonism — an extrapyramidal motor disorder defined by the tetrad of rigidity, tremor, hypokinesia/bradykinesia, and postural instability, with secondary defective posture/gait, mask-like face, and sialorrhoea. (KDT 8e Ch.31, p.452)
- Bradykinesia — must be present for a diagnosis of Parkinson's disease; focal dystonic features may also be present. (Katzung 16e Ch.28, p.518)
- Pathological hallmark — loss of pigmented dopaminergic neurones of the substantia nigra pars compacta (SN-PC) with intracellular Lewy bodies. (G&G 14e Ch.21, p.413)
- Lewy bodies — intracellular inclusions whose principal aggregated component is α-synuclein; PD is now recognised as a synucleinopathy. (G&G 14e Ch.21, p.414)
- Threshold for symptoms — loss of 70–80 % of DA-containing SN-PC neurones accompanies symptomatic PD. (G&G 14e Ch.21, p.415)
- Natural history — untreated PD progresses over 5–10 years to a rigid, akinetic state; death usually from aspiration pneumonia or pulmonary embolism. (Katzung 16e Ch.28, p.518)
- Pharmacotherapy impact — drugs do not change the underlying course but provide ~5–10 years of additional productive life and lower mortality when initiated early. (KDT 8e Ch.31, p.460; G&G 14e Ch.21, p.415)
- Wilson's disease — (hepatolenticular degeneration; chronic copper poisoning) is a rare cause of parkinsonism. (KDT 8e Ch.31, p.452)
- Drug-induced parkinsonism — (reversible) due to neuroleptics and metoclopramide (D2 blockers) is now common; reserpine-induced (DA depleter) is historical. (KDT 8e Ch.31, p.452)
2. Non-motor manifestations
- Wider involvement — PD affects brainstem, hippocampus, neocortex beyond the dopaminergic system. (G&G 14e Ch.21, p.415)
- Premotor (preclinical) — hyposmia/anosmia, REM-sleep behaviour disorder, constipation, depression, anxiety — may precede motor symptoms by years. (G&G 14e Ch.21, p.415; Katzung 16e Ch.28, p.518)
- Cognitive features — impaired attention, hallucinations, delusions, executive and visuospatial dysfunction; dementia accompanies advanced disease. (G&G 14e Ch.21, p.415)
- Autonomic dysfunction — sphincter or sexual dysfunction, dysphagia/choking, sweating abnormalities, sialorrhoea, BP dysregulation. (Katzung 16e Ch.28, p.518)
- Affective symptoms — anxiety, depression, apathy, fatigue; sensory complaints and pain are recognised non-motor features. (Katzung 16e Ch.28, p.518)
- Braak staging — stage 1 olfactory bulb/medulla → stage 2 pons → stage 3 midbrain (incl. SN-PC, motor symptoms emerge) → stage 4 mesocortex/thalamus → stages 5–6 neocortex. (Katzung 16e Ch.28, p.519)
3. Pathogenesis & etiology
- Multifactorial cause — ageing + genetic predisposition + oxidative free-radical generation + environmental MPTP-like toxins + excitotoxic NMDA-mediated Ca2+ overload. (KDT 8e Ch.31, p.452)
- Pathogenic mechanisms — impaired protein degradation, intracellular protein accumulation, oxidative stress, mitochondrial damage, inflammatory cascades, apoptosis. (Katzung 16e Ch.28, p.518)
- Twin studies — genetic factors are most important when PD presents under age 50. (Katzung 16e Ch.28, p.518)
- Genetic abnormalities — account for 10–15 % of PD cases. (Katzung 16e Ch.28, p.518)
- Autosomal-dominant genes — SNCA (α-synuclein, 4q21) — point mutations or duplication/triplication; LRRK2 (12cen) — most common AD form, gain-of-kinase function; UCHL1. (Katzung 16e Ch.28, p.518; G&G 14e Ch.21, p.413)
- Autosomal-recessive (early-onset) — PARK2/Parkin (E3 ubiquitin ligase loss-of-function); DJ-1 and PINK1 (mitochondrial quality-control proteins). (Katzung 16e Ch.28, p.518; G&G 14e Ch.21, p.413)
- Risk-modifier genes — α-synuclein, LRRK2, MAPT (tau), GBA (β-glucocerebrosidase). (G&G 14e Ch.21, p.413)
- GBA mutations — heterozygous GBA mutations are the strongest single common genetic risk factor for PD; not in KDT. (G&G 14e Ch.21, p.414)
- Protective epidemiologic factors — cigarette smoking, coffee, anti-inflammatory drug use, high serum uric acid. (Katzung 16e Ch.28, p.518)
- Risk factors — teaching, healthcare, farming professions; lead or manganese exposure; vitamin D deficiency; pesticide exposure. (Katzung 16e Ch.28, p.518; G&G 14e Ch.21, p.414)
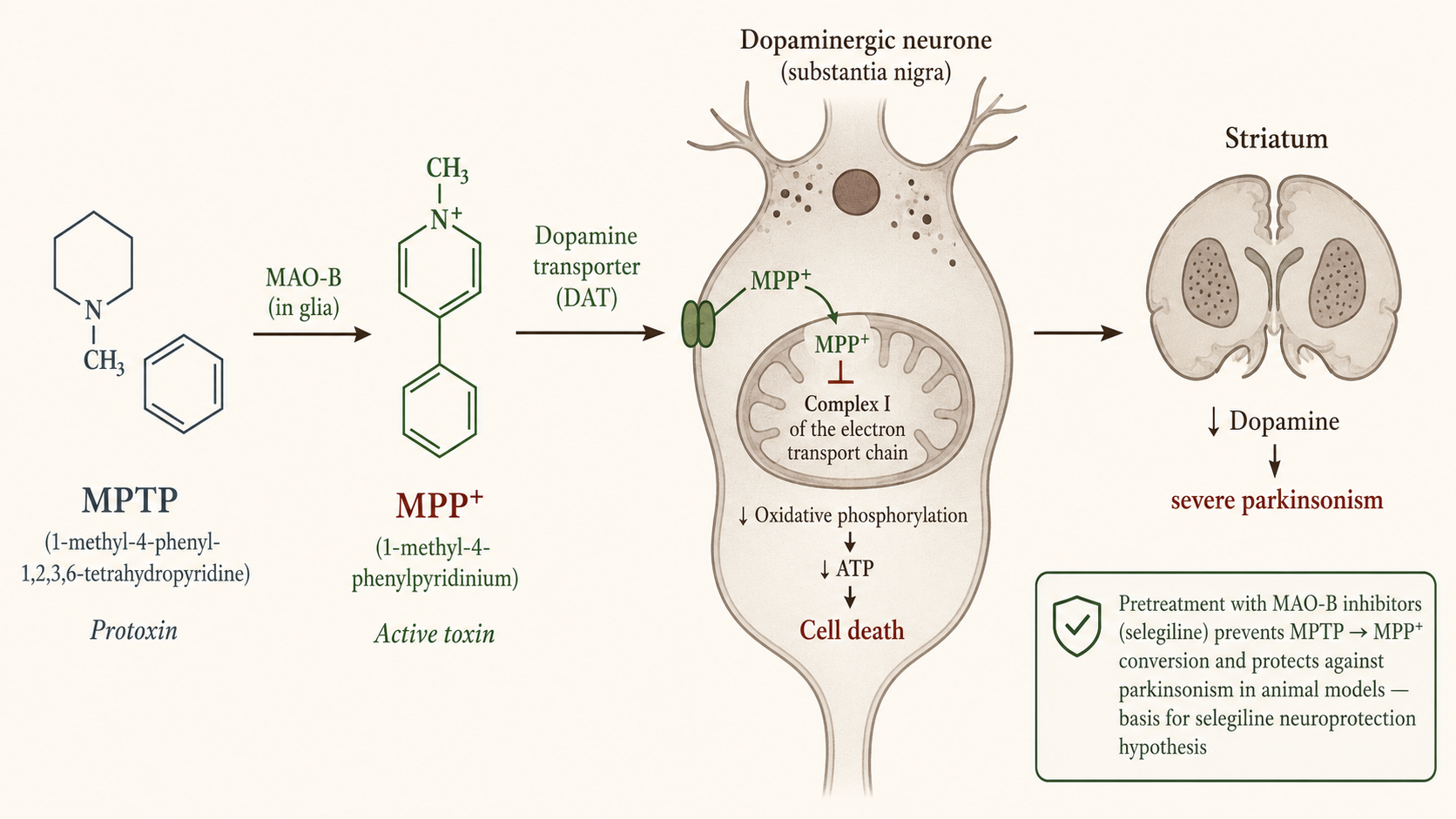
- MPTP — 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine — a protoxin that opened the field of PD experimental models in 1983. (Katzung 16e Ch.28, p.530)
- MPTP mechanism — MPTP → (MAO-B oxidation) → MPP+; MPP+ concentrated in SN-PC neurones via DAT; inhibits mitochondrial complex I → halts oxidative phosphorylation → cell death → striatal DA depletion → severe parkinsonism. (Katzung 16e Ch.28, p.530)
- Selegiline rationale — prophylactic MAO-B inhibition prevents MPTP → MPP+ conversion and protects animals — basis for trials of selegiline/rasagiline as putative neuroprotective agents. (Katzung 16e Ch.28, p.530)
- Prion-like spread — Lewy bodies in fetal dopaminergic transplants placed years earlier support the hypothesis that PD may behave as a prion-like spreading proteinopathy. (Katzung 16e Ch.28, p.518)
- α-Synuclein SAA — spinal-fluid seed amplification assay has high sensitivity/specificity for distinguishing PD from controls and may serve as a pre-symptomatic biomarker. (Katzung 16e Ch.28, p.528)
4. Neurochemistry — dopamine system
- Core lesion — degeneration of the nigrostriatal (dopaminergic) tract from SN-PC → DA deficiency in striatum which controls muscle tone and coordinates movement. (KDT 8e Ch.31, p.452)
- DA imbalance hypothesis — loss of inhibitory dopaminergic input creates an imbalance between dopaminergic (inhibitory) and cholinergic (excitatory) systems in the striatum; cholinergic system is not primarily affected but its suppression by anticholinergics restores balance. (KDT 8e Ch.31, p.452)
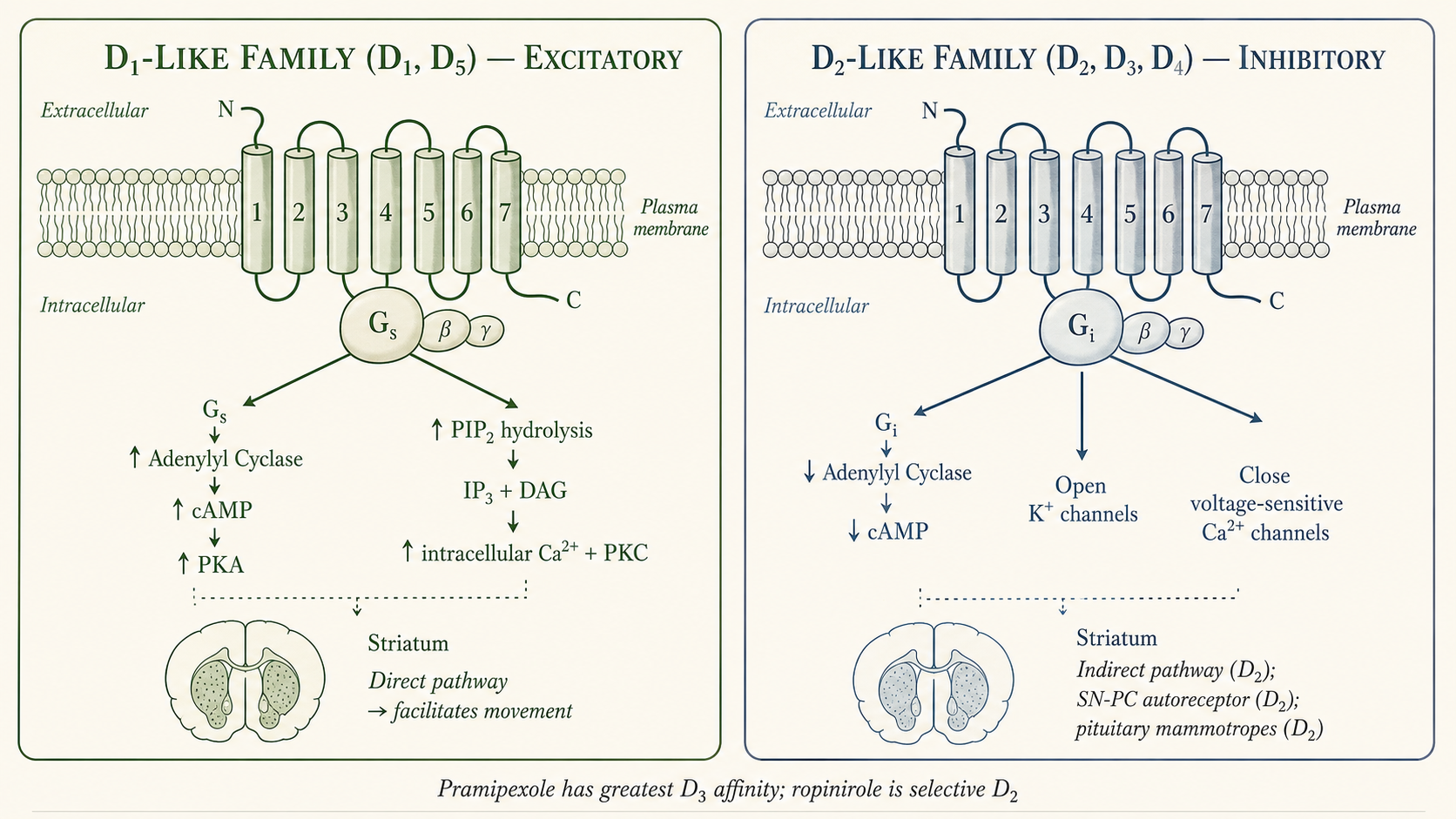
- DA receptor subtypes — five (D1–D5), all GPCRs, two families. (KDT 8e Ch.31, p.453; G&G 14e Ch.21, p.415)
- D1-like family (D1, D5) — excitatory; Gs-coupled → ↑ adenylyl cyclase → ↑ cAMP; also ↑ PIP2 hydrolysis → ↑ intracellular Ca2+ + PKC via IP3 and DAG. (KDT 8e Ch.31, p.453)
- D2-like family (D2, D3, D4) — inhibitory; Gᵢ-coupled → ↓ adenylyl cyclase, open K+ channels, depress voltage-sensitive Ca2+ channels. (KDT 8e Ch.31, p.453)
- Receptor distribution — D1 + D2 both abundant in striatum (most relevant to PD therapy); D2 in SN-PC and pituitary mammotropes; D3 in nucleus accumbens and hypothalamus; D4, D5 mostly in neocortex, midbrain, medulla, hippocampus. (G&G 14e Ch.21, p.415; KDT 8e Ch.31, p.453)
- Both D1 and D2 — involved in the therapeutic response to levodopa despite opposite cellular effects, because they regulate two pathways with opposite effects on thalamocortical drive. (KDT 8e Ch.31, p.453)
- Therapeutic relevance — antiparkinsonian benefit appears mostly D2-mediated, but D1 stimulation may be required for maximal benefit. (Katzung 16e Ch.28, p.519)
- D3-selective agonists — (pramipexole) developed; D3 implicated in mood and impulse-control behaviours of DA agonist therapy. (Katzung 16e Ch.28, p.524)
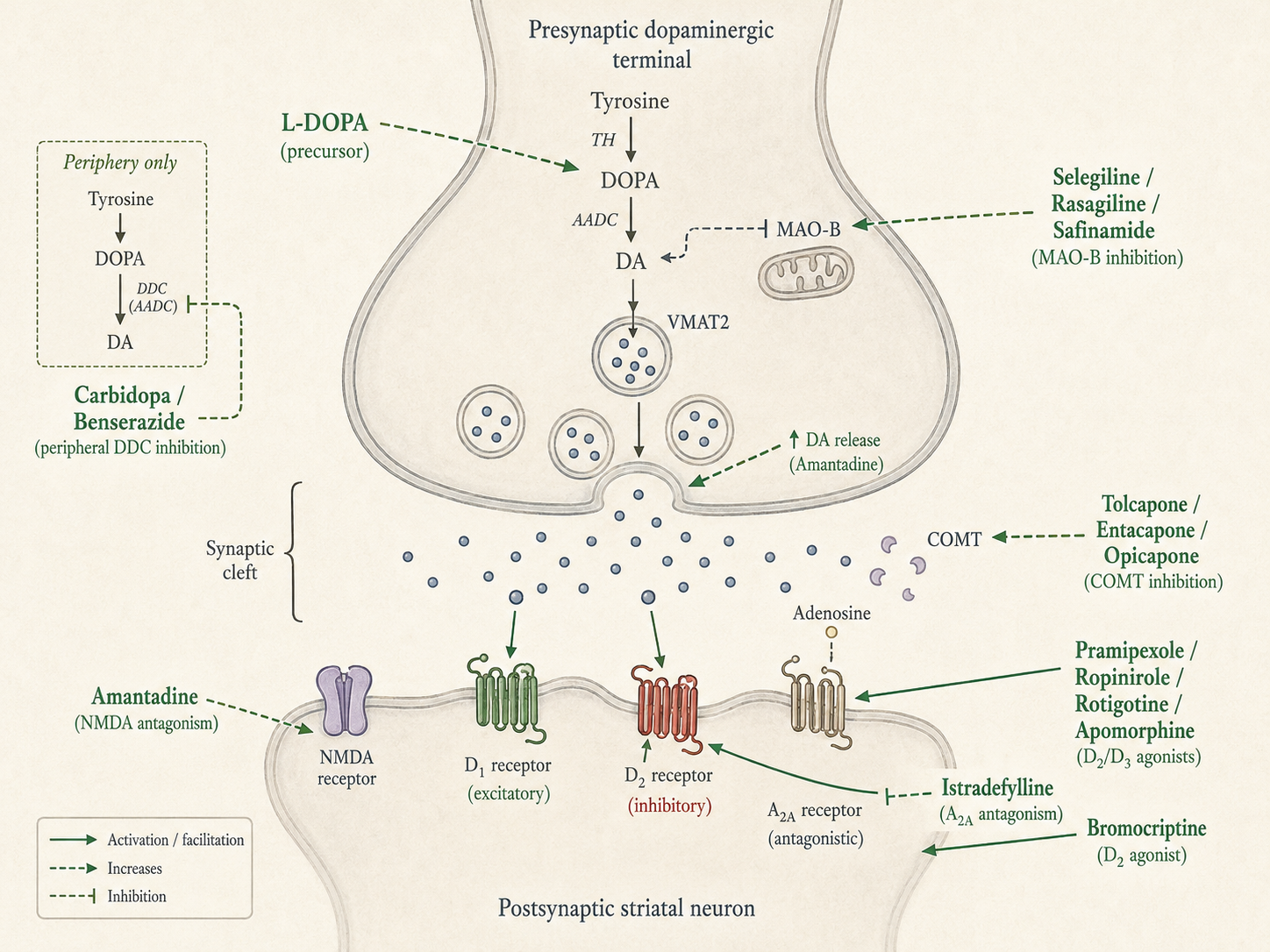
- DA synthesis — phenylalanine → (PAH, hepatic) → tyrosine → (TH, rate-limiting) → l-DOPA → (AADC) → dopamine → vesicles via VMAT2. (G&G 14e Ch.21, p.416)
- DA metabolism — synaptic DA → DAT/NET reuptake or postsynaptic OCT3 → cytosolic DA → MAO + ALDH (intraneuronal) and COMT + MAO/ALDH (non-neuronal) → final metabolite HVA. (G&G 14e Ch.21, p.416)
- Other neurotransmitters — noradrenaline and serotonin also reduced in PD brain — clinical relevance uncertain. (Katzung 16e Ch.28, p.519)
5. Basal-ganglia circuitry & pathophysiology of motor symptoms
- Modulatory side-loop — basal ganglia regulate flow of information from cerebral cortex to spinal motor neurones; striatum (caudate + putamen) is the principal input structure. (G&G 14e Ch.21, p.415; KDT 8e Ch.31, p.453)
- Striatal cells — projection neurones are GABAergic medium spiny neurones; small but important interneurones use acetylcholine and neuropeptides. (G&G 14e Ch.21, p.415)
- Striatal inputs — excitatory glutamatergic from motor cortex; modulatory dopaminergic from SN-PC; balancing cholinergic interneurones. (KDT 8e Ch.31, p.453)
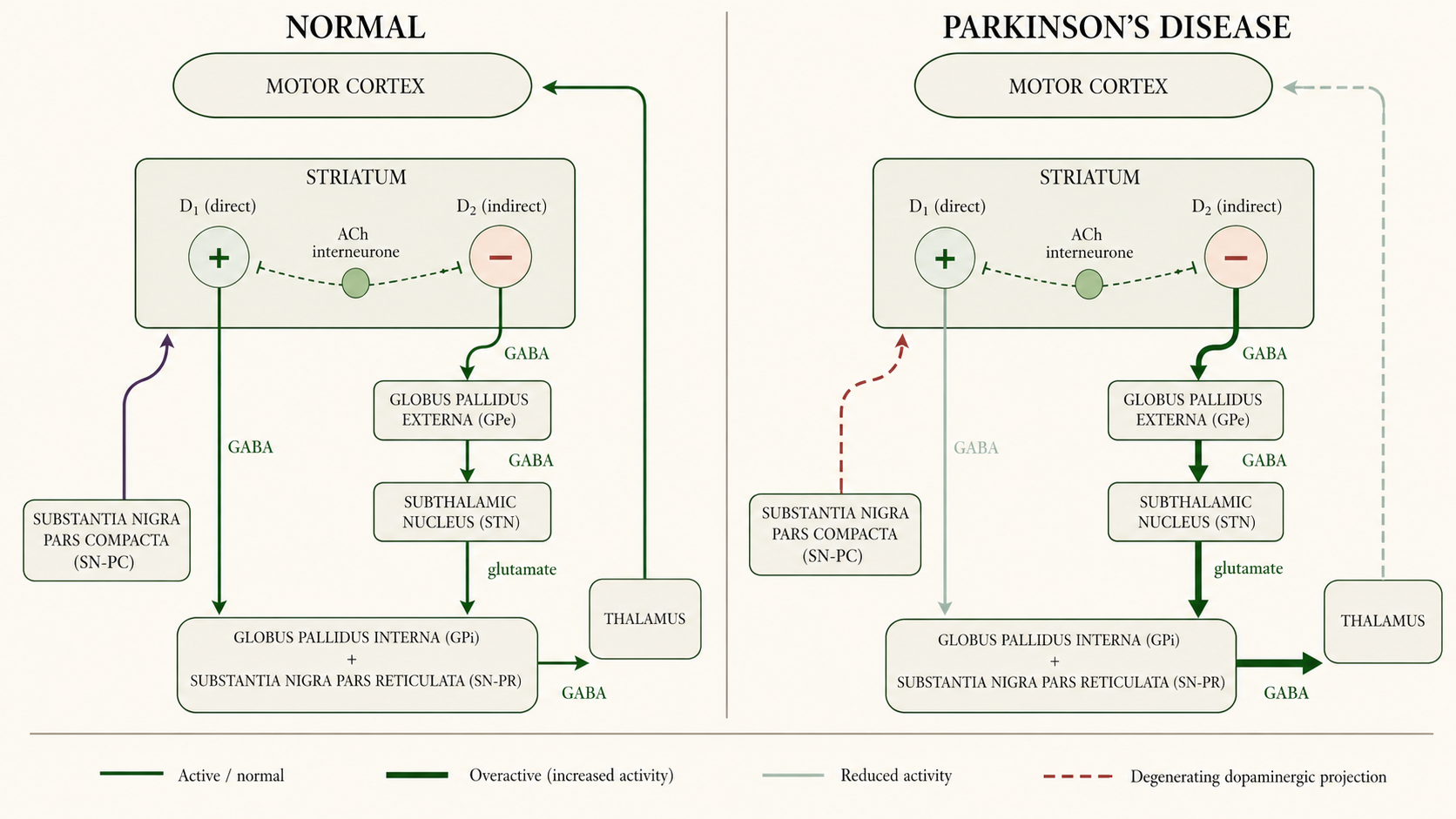
- Direct pathway — striatum → SN-PR / GP-I (single GABAergic inhibitory link); striatal neurones express excitatory D1 receptors. (KDT 8e Ch.31, p.454; G&G 14e Ch.21, p.415)
- Indirect pathway — striatum → GP-E → STN → SN-PR / GP-I; two GABAergic inhibitory relays + one excitatory glutamatergic terminal from STN; striatal neurones express inhibitory D2 receptors. (KDT 8e Ch.31, p.454; G&G 14e Ch.21, p.415)
- Output — SN-PR + GP-I are GABAergic → VA/VL thalamus → glutamatergic feedback to motor cortex. (G&G 14e Ch.21, p.415)
- Net effect of striatal DA — stimulates D1-direct pathway → ↑ inhibition of SN-PR/GP-I → disinhibits thalamus → ↑ cortical drive; inhibits D2-indirect pathway → ↓ STN drive → ↓ SN-PR/GP-I → again disinhibits thalamus. Both pathways converge to facilitate movement and reduce muscle tone. (KDT 8e Ch.31, p.454; Katzung 16e Ch.28, p.519)
- In PD — loss of nigrostriatal DA → ↓ direct-pathway activity + ↑ indirect-pathway activity → ↑ inhibitory output from SN-PR/GP-I → ↓ thalamocortical drive → bradykinesia. (G&G 14e Ch.21, p.415)
- Model limitations — does not adequately explain rest tremor or levodopa-induced dyskinesia; anatomy is more complex with multiple co-transmitters. (G&G 14e Ch.21, p.415)
- Surgical-target rationale — model predicts that lesioning or stimulating STN or GP-I should reduce excessive inhibitory output and restore motor function — borne out by DBS results. (Katzung 16e Ch.28, p.527)
6. Classification of antiparkinsonian drugs
Drugs affecting brain dopaminergic system
- DA precursor — Levodopa.
- Peripheral decarboxylase inhibitors (adjuvants) — Carbidopa, Benserazide.
- Dopaminergic agonists — ergot derivatives — Bromocriptine, Pergolide.
- Non-ergot oral — Pramipexole, Ropinirole.
- Non-ergot transdermal — Rotigotine.
- Non-ergot injectable (rescue) — Apomorphine.
- MAO-B inhibitors — Selegiline, Rasagiline, Safinamide.
- COMT inhibitors — Entacapone, Tolcapone, Opicapone.
- NMDA antagonist / DA facilitator — Amantadine.
- Adenosine A2A receptor antagonist — Istradefylline.
Drugs affecting brain cholinergic system
- Central anticholinergics — Trihexyphenidyl (benzhexol), Procyclidine, Biperiden, Benztropine.
- Antihistaminics with central anticholinergic action — Orphenadrine, Promethazine, Diphenhydramine. (KDT 8e Ch.31, p.453)
7. Levodopa — overview & mechanism
- Chemical identity — (–)-3-(3,4-dihydroxyphenyl)-l-alanine — levorotatory stereoisomer of dopa, immediate metabolic precursor of DA. (G&G 14e Ch.21, p.415)
- Most efficacious single agent — in PD; efficacy exceeds any other antiparkinsonian drug used alone. (KDT 8e Ch.31, p.452)
- 1967 breakthrough — Cotzias produced dramatic improvement based on prior work showing DA depletion in PD striatum and reversal of reserpine-induced motor defect by DOPA. (KDT 8e Ch.31, p.452)
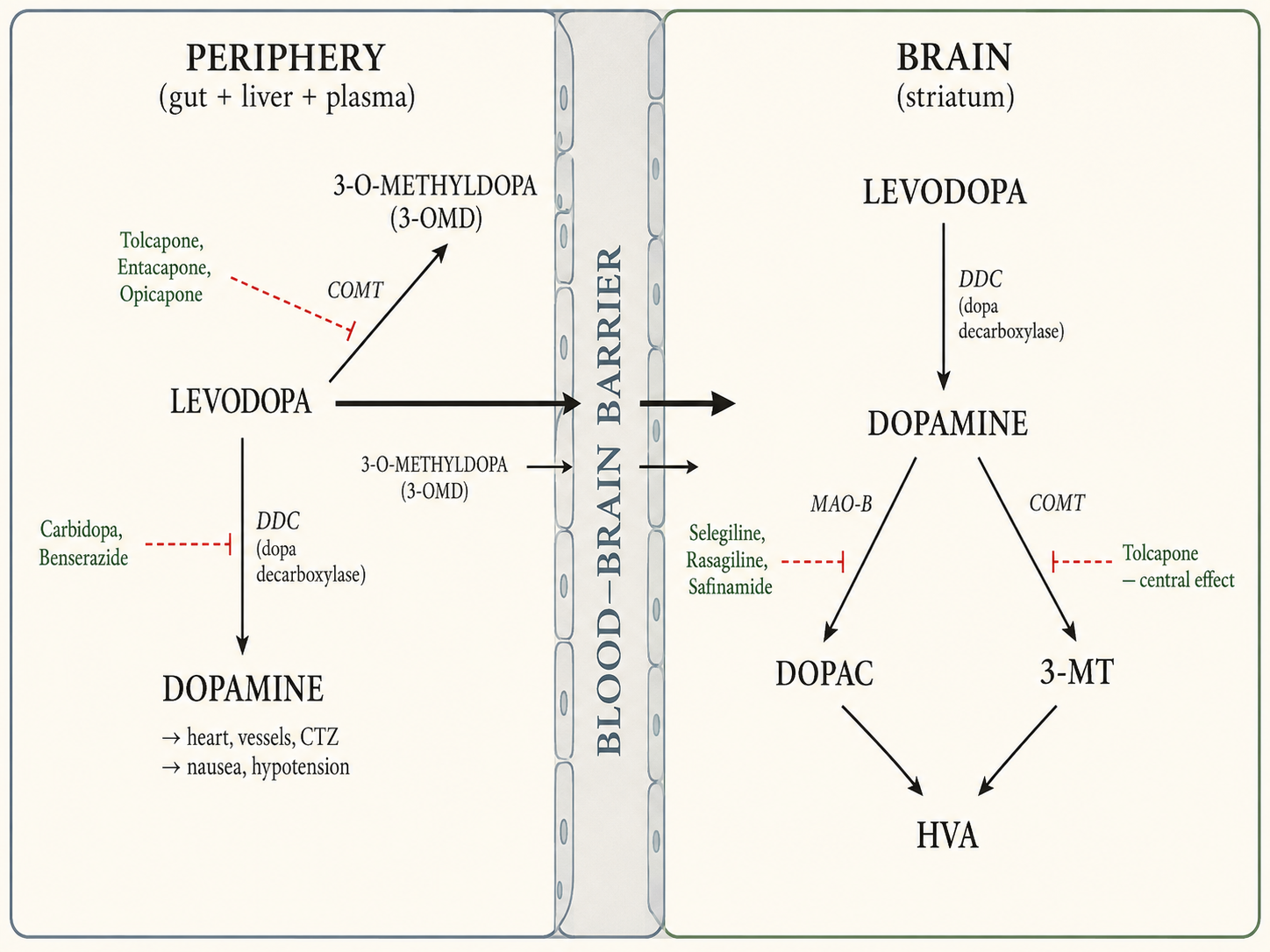
- Why not give DA directly — DA does not cross BBB; levodopa crosses via L-aromatic amino acid transporter (LAT). (G&G 14e Ch.21, p.415; KDT 8e Ch.31, p.452)
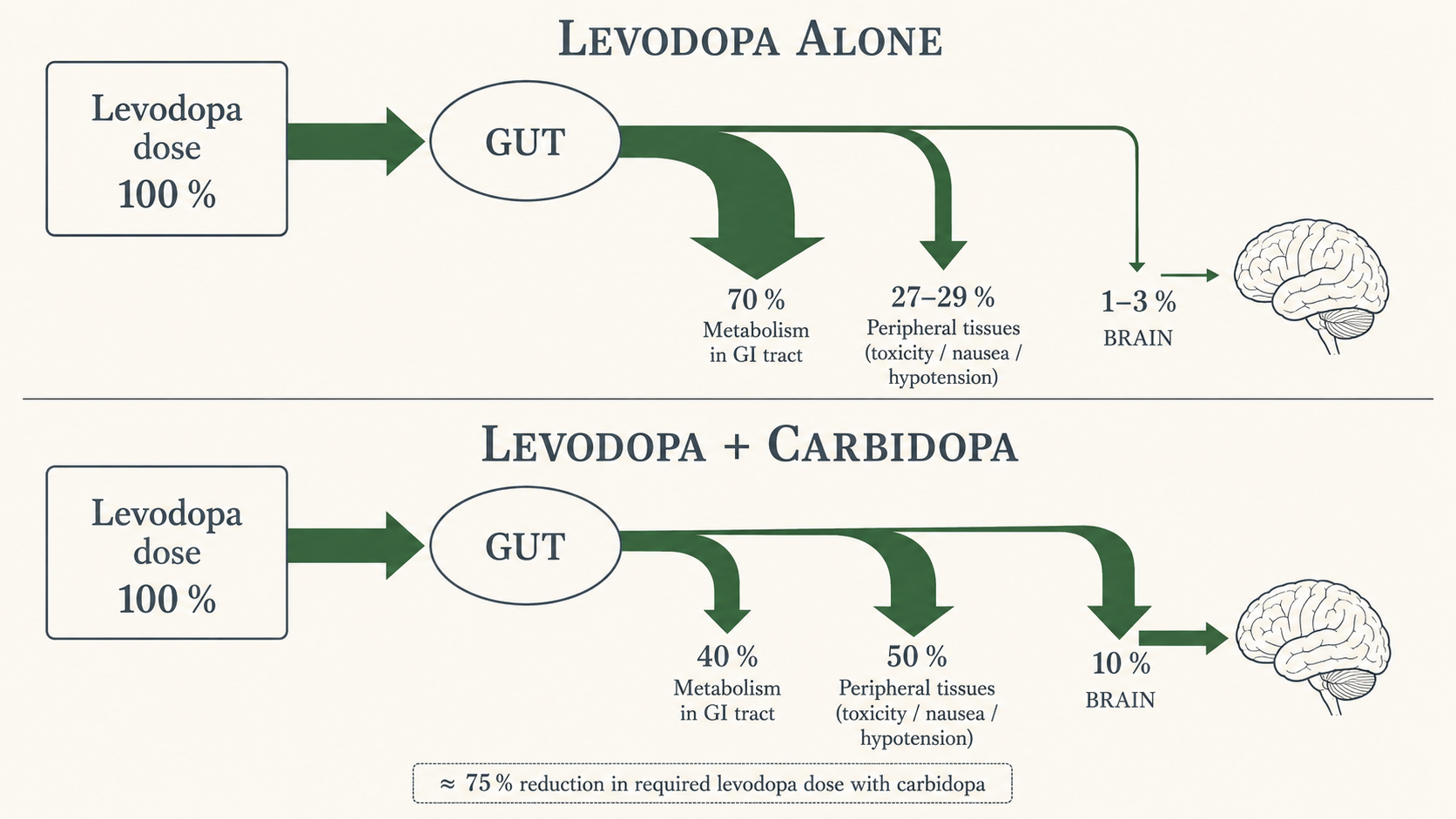
- Fate without DDC inhibitor — >95 % decarboxylated peripherally (gut + liver); only 1–2 % crosses BBB (KDT) / 1–3 % (G&G/Katzung) — minor numerical disagreement; figure is approximate. (KDT 8e Ch.31, p.452; G&G 14e Ch.21, p.415)
- Sites of peripheral DA action — heart, vessels, peripheral organs, CTZ (the chemoreceptor trigger zone is in floor of IV ventricle but is outside BBB). (KDT 8e Ch.31, p.453)
- Central conversion — levodopa entering brain is taken up by surviving dopaminergic neurones, decarboxylated to DA, stored in vesicles, and released as transmitter. (KDT 8e Ch.31, p.453)
- Buffering capacity — surviving terminals essential for stable benefit — they buffer rapid changes in plasma levodopa; loss of buffering drives motor fluctuations. (G&G 14e Ch.21, p.416)
8. Levodopa — pharmacological actions
8.1 CNS
- Selective effect — little effect in normal individuals or in non-PD neurological disease — selectively reverses the deficit in PD. (KDT 8e Ch.31, p.453)
- Order of improvement — hypokinesia and rigidity first, tremor later; secondary symptoms (posture, gait, handwriting, speech, facial expression, mood, self-care) gradually normalised. (KDT 8e Ch.31, p.453)
- Therapeutic ceiling — benefit nearly complete in early disease but declines as disease advances. (KDT 8e Ch.31, p.453)
- Dementia — if present, does not improve with levodopa and predisposes to psychiatric symptoms. (KDT 8e Ch.31, p.453)
8.2 CVS
- Tachycardia — from peripheral DA via β-adrenergic action. (KDT 8e Ch.31, p.454)
- BP not raised — despite vascular adrenergic stimulation — instead postural hypotension is common (probable central action: ↓ sympathetic outflow from excess central DA/NA). (KDT 8e Ch.31, p.454)
- Ganglionic effect — peripheral DA in autonomic ganglia may impede ganglionic transmission. (KDT 8e Ch.31, p.454)
- Tolerance — develops to both cardiac stimulant and hypotensive actions. (KDT 8e Ch.31, p.454)
- Arrhythmias — tachycardia, ventricular extrasystoles, rarely atrial fibrillation; incidence low and reduced further by carbidopa coadministration. (Katzung 16e Ch.28, p.521)
8.3 CTZ
- Nausea / vomiting — DA is excitatory at CTZ → nausea and vomiting in ~80 % on levodopa monotherapy; tolerance develops gradually. (KDT 8e Ch.31, p.454; Katzung 16e Ch.28, p.520)
- With carbidopa — incidence falls to <20 %. (Katzung 16e Ch.28, p.521)
8.4 Endocrine
- Prolactin — DA acts on pituitary mammotropes → ↓ serum prolactin during levodopa therapy. (KDT 8e Ch.31, p.454)
- GH — ↑ GH release in normals; GH is not increased in parkinsonian patients — regulation appears altered. (KDT 8e Ch.31, p.454)
9. Levodopa — pharmacokinetics
- Absorption — rapid from small intestine via active transport for aromatic amino acids. (KDT 8e Ch.31, p.455; G&G 14e Ch.21, p.415)
- Bioavailability — gastric emptying — slow emptying ↑ exposure to gut-wall + hepatic degrading enzymes → less reaches BBB. (KDT 8e Ch.31, p.455)
- Bioavailability — gastric pH — affects absorption. (Katzung 16e Ch.28, p.520)
- Dietary amino acids — compete with levodopa for the same carrier — blood levels lower with high-protein meals; the same carrier limits BBB transport. (KDT 8e Ch.31, p.455; G&G 14e Ch.21, p.416)
- Tmax — peak plasma 0.5–2 h after oral dose. (Katzung 16e Ch.28, p.520; G&G 14e Ch.21, p.416)
- Plasma t½ — 1–2 h (KDT) / 1–3 h (Katzung & G&G); inter-individual variability is wide. (KDT 8e Ch.31, p.455; Katzung 16e Ch.28, p.520)
- Pyridoxal — cofactor for dopa decarboxylase — explains pyridoxine interaction. (KDT 8e Ch.31, p.455)
- Excretion — ~⅔ of dose appears in urine as metabolites within 8 h, mainly HVA and DOPAC after conjugation. (Katzung 16e Ch.28, p.520; KDT 8e Ch.31, p.455)
- Periphery — levodopa ⇌ 3-O-methyldopa (3-OMD via COMT); levodopa → DA via DDC → DOPAC (MAO/ALDH) → HVA (COMT). (KDT 8e Ch.31, p.455)
- Brain — 3-OMD via COMT; levodopa → DA via DDC; DA → 3-MT (COMT) and DOPAC (MAO-B/ALDH) → both → HVA. (KDT 8e Ch.31, p.455)
- 3-OMD competition — high 3-OMD levels reduce levodopa entry by competing for active BBB transport. (Katzung 16e Ch.28, p.526)
10. Levodopa — adverse effects
10.1 At initiation (early, dose-related, reversible)
- Nausea & vomiting — in nearly every patient on monotherapy (~80 %); minimised by starting low, dividing doses, taking with meals; tolerance develops. (KDT 8e Ch.31, p.455; Katzung 16e Ch.28, p.520)
- Postural hypotension — in ~⅓; mostly asymptomatic; some experience dizziness or syncope; worse with antihypertensives; tolerance develops. (KDT 8e Ch.31, p.455)
- Cardiac arrhythmias — β-adrenergic action of peripheral DA; more in pre-existing heart disease. (KDT 8e Ch.31, p.456)
- Angina — exacerbation in patients with pre-existing ischaemic heart disease. (KDT 8e Ch.31, p.456)
- Taste alteration — may occur. (KDT 8e Ch.31, p.456)
- Hypertension — with massive doses, with non-selective MAOIs, or with sympathomimetics. (Katzung 16e Ch.28, p.522)
10.2 With prolonged therapy — motor complications
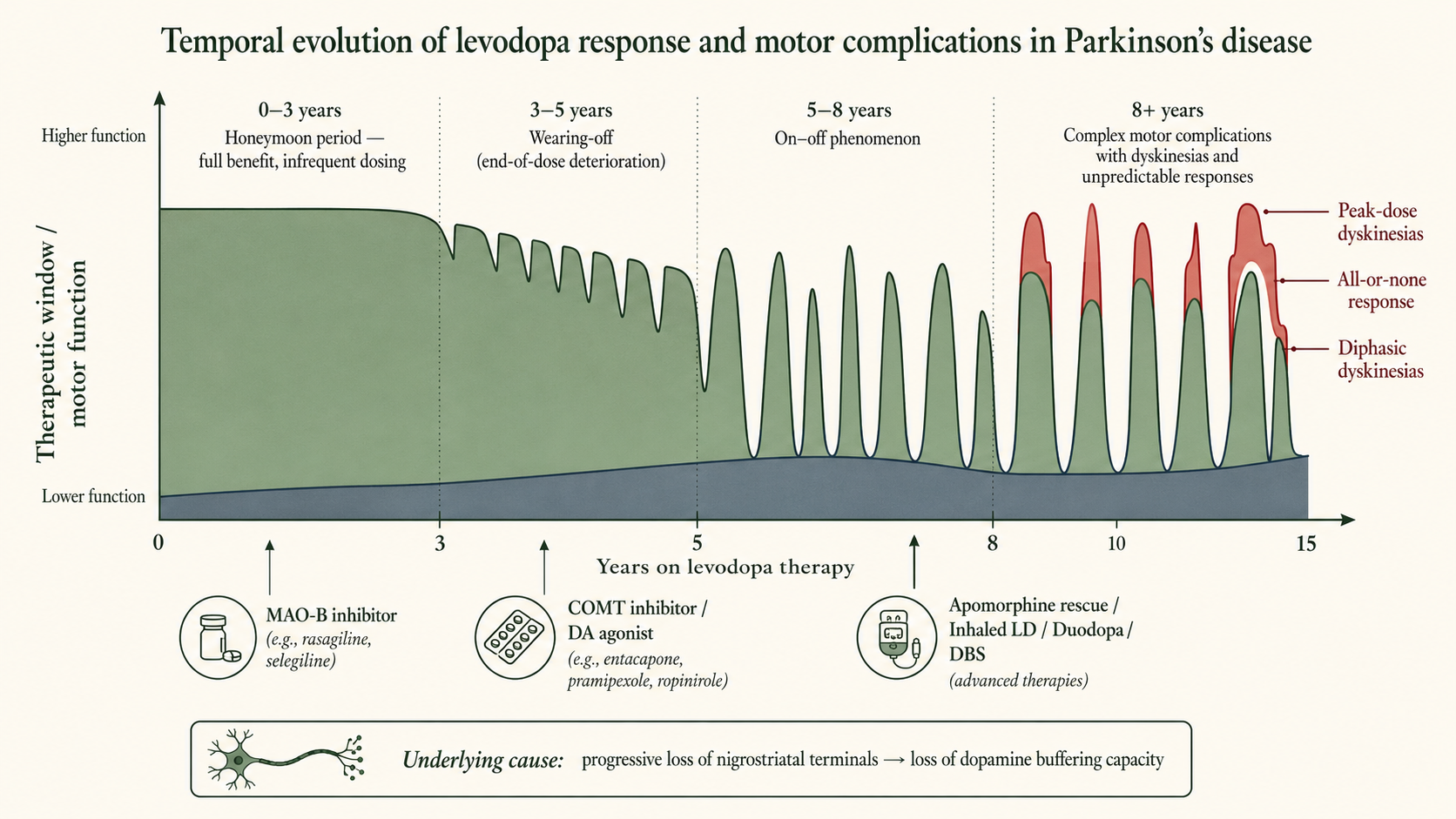
- Dyskinesias — abnormal involuntary movements — facial tics, grimacing, tongue thrusting, choreoathetoid limb movements. (KDT 8e Ch.31, p.456)
- Incidence — up to 80 % of patients receiving levodopa for >10 years. (Katzung 16e Ch.28, p.522)
- Onset — after a few months at therapeutic dose; intensity correlates with plasma levodopa levels; no tolerance develops. (KDT 8e Ch.31, p.456)
- Phenotype — choreoathetosis of face and distal extremities is most common; pattern tends to be constant within an individual. (Katzung 16e Ch.28, p.522)
- Pathogenesis — unclear; hypotheses include unequal striatal DA distribution and dopaminergic denervation + chronic pulsatile receptor stimulation. (Katzung 16e Ch.28, p.522)
- Continuous delivery — lower incidence with intraduodenal/intrajejunal infusion or transdermal patch — supports the pulsatile-stimulation hypothesis. (Katzung 16e Ch.28, p.522)
- Diphasic dyskinesias — occur as patient comes on and again as benefit wears off; managed by smaller, more frequent doses or substituting some levodopa with a DA agonist. (Katzung 16e Ch.28, p.522)
10.3 Response fluctuations
- Wearing-off — end-of-dose deterioration: gradual loss of benefit before next dose; progresses with disease. (KDT 8e Ch.31, p.456)
- On–off phenomenon — rapid, unpredictable switches between mobility (on) and akinesia (off), often with dyskinesia during on-state. (KDT 8e Ch.31, p.456)
- All-or-none — develops over years — patient alternately well and disabled; abnormal movements may jeopardise even the on-phase. (KDT 8e Ch.31, p.456)
- Mechanism — progressive degeneration of DA neurones with loss of buffering capacity → moment-to-moment striatal DA synthesis is unstable. (KDT 8e Ch.31, p.456)
- Management strategies — dose fractionation, more frequent dosing, evening protein meal, longer-acting / controlled-release formulations, COMT inhibitors, MAO-B inhibitors, DA agonists, apomorphine rescue, inhaled levodopa, surgery. (Katzung 16e Ch.28, p.522)
10.4 Behavioural / psychiatric
- Spectrum — mild anxiety, nightmares to severe depression, mania, hallucinations, mental confusion, frank psychosis. (KDT 8e Ch.31, p.456)
- Mechanism — excessive DA action in limbic system (antidopaminergics are antipsychotic). (KDT 8e Ch.31, p.456)
- With carbidopa — more common (higher central levels); may be precipitated by intercurrent illness or surgery. (Katzung 16e Ch.28, p.522)
- Contraindication — levodopa is contraindicated in patients with psychotic illness. (KDT 8e Ch.31, p.456)
- More likely culprits — confusion and hallucinations developing in PD patients are more likely due to anticholinergics, amantadine, or DA agonists than to levodopa itself. (Katzung 16e Ch.28, p.522)
- Dopamine dysregulation syndrome — compulsive overuse of dopaminergic medication + other impulsive behaviours; more common with DA agonists. (Katzung 16e Ch.28, p.522)
- Punding — stereotyped, complex but purposeless motor activity (sorting/lining objects, repetitive grooming); responds to dose reduction or atypical antipsychotics. (Katzung 16e Ch.28, p.522)
- Atypical antipsychotics of choice — low D2 affinity — clozapine, quetiapine, olanzapine, risperidone; clozapine and quetiapine considered most effective and best tolerated. (Katzung 16e Ch.28, p.522; G&G 14e Ch.21, p.418)
- Pimavanserin — selective serotonin 5-HT2a inverse agonist 34 mg/day; FDA-approved for PD psychosis; avoid in QT prolongation; contraindicated for dementia-related psychosis. (Katzung 16e Ch.28, p.522)
- Black-box warning — increased mortality in elderly with dementia-related psychosis treated with antipsychotics. (G&G 14e Ch.21, p.421)
- Suicidality — appears increased in PD; whether disease- or treatment-related is uncertain. (G&G 14e Ch.21, p.418)
- Conventional D2 blockers — phenothiazines, haloperidol — contraindicated; worsen parkinsonism. (G&G 14e Ch.21, p.418)
10.5 Miscellaneous adverse effects
- Mydriasis — may precipitate acute angle-closure glaucoma in susceptible eyes. (Katzung 16e Ch.28, p.522)
- Various — blood dyscrasias; positive Coombs' test with haemolysis; hot flushes; aggravation of gout; abnormalities of smell or taste. (Katzung 16e Ch.28, p.522)
- Discoloration — brownish saliva, urine, vaginal secretions. (Katzung 16e Ch.28, p.522)
- Other — priapism (rare); transient ↑ blood urea, transaminases, alkaline phosphatase, bilirubin. (Katzung 16e Ch.28, p.522)
10.6 Cautions / contraindications
- Cautious use — elderly; ischaemic heart disease, cerebrovascular disease, psychiatric illness, hepatic and renal disease, peptic ulcer (bleeding risk), glaucoma, gout. (KDT 8e Ch.31, p.456)
- Contraindicated — angle-closure glaucoma, active psychosis, history of melanoma or suspicious skin lesions (levodopa is a precursor of melanin and may theoretically activate melanoma). (Katzung 16e Ch.28, p.523)
- Open-angle glaucoma — acceptable if IOP is controlled and monitored. (Katzung 16e Ch.28, p.523)
- Drug holidays — (3–21-day discontinuation) no longer recommended — risks of aspiration pneumonia, VTE, depression; benefit temporary. (KDT 8e Ch.31, p.461; Katzung 16e Ch.28, p.522)
- Abrupt withdrawal — of levodopa or DA agonists may precipitate a state resembling neuroleptic malignant syndrome with rigidity, hyperthermia, mental deterioration. (KDT 8e Ch.31, p.461; Katzung 16e Ch.28, p.525)
11. Levodopa — drug interactions
- Pyridoxine (B6) — abolishes the therapeutic effect of levodopa monotherapy by enhancing peripheral decarboxylation; does NOT abolish effect when carbidopa coadministered. (KDT 8e Ch.31, p.456; G&G 14e Ch.21, p.420)
- Phenothiazines, butyrophenones, metoclopramide — reverse therapeutic effect by blocking D2 receptors; antiemetics of these classes should be avoided. (KDT 8e Ch.31, p.456)
- Domperidone — blocks levodopa-induced nausea/vomiting WITHOUT abolishing antiparkinsonian effect because it does not cross BBB but reaches the CTZ (which is outside BBB) — useful clinical exploitation. (KDT 8e Ch.31, p.456)
- Reserpine — abolishes levodopa action by preventing entry of newly formed DA into synaptic vesicles (VMAT2 blockade). (KDT 8e Ch.31, p.456)
- Non-selective MAO inhibitors — prevent peripheral degradation of DA/NA → potential hypertensive crisis; discontinue ≥14 days before levodopa. (KDT 8e Ch.31, p.456; Katzung 16e Ch.28, p.523)
- Antihypertensives — postural hypotension accentuated; reduce antihypertensive dose if levodopa started. (KDT 8e Ch.31, p.457)
- Atropine and antiparkinsonian anticholinergics — additive therapeutic action with low-dose levodopa, but retard absorption (slow gastric emptying) → ↑ peripheral degradation → reduced efficacy; not a problem with carbidopa coadministration. (KDT 8e Ch.31, p.457)
12. Levodopa — preparations & dosing (Indian context)
- Initiation — 0.25 g BD after meals; increase gradually to 2–3 g/day for monotherapy. (KDT 8e Ch.31, p.456)
- Indian brands — LEVOPA, BIDOPAL 0.5 g tab. (KDT 8e Ch.31, p.456)
- Standard practice — combination with carbidopa; pure levodopa is reserved for patients with intolerable dyskinesias on the combination. (KDT 8e Ch.31, p.461)
13. Carbidopa & Benserazide
- Mechanism — extracerebral dopa decarboxylase (DDC) inhibitors that do NOT cross BBB → do not inhibit central DA synthesis. (KDT 8e Ch.31, p.456)
- Benefit 1 — prolongs plasma t½ of levodopa. (KDT 8e Ch.31, p.457)
- Benefit 2 — reduces required levodopa dose by ~75–80 % (~¼ of monotherapy dose). (KDT 8e Ch.31, p.457; G&G 14e Ch.21, p.416)
- Benefit 3 — ↓ peripheral DA → ↓ nausea, vomiting, cardiac complications → therapeutic doses attained more quickly. (KDT 8e Ch.31, p.457)
- Benefit 4 — eliminates pyridoxine reversal. (KDT 8e Ch.31, p.457)
- Benefit 5 — smoother cerebral DA levels → ↓ on–off effect. (KDT 8e Ch.31, p.457)
- Benefit 6 — some non-responders to levodopa monotherapy do respond to combination. (KDT 8e Ch.31, p.457)
- Problem 1 — involuntary movements may be more pronounced and appear earlier. (KDT 8e Ch.31, p.457)
- Problem 2 — behavioural abnormalities; excessive day-time sleepiness in some; postural hypotension. (KDT 8e Ch.31, p.457)
- Carbidopa dose — ~75 mg/day saturates peripheral DDC and prevents nausea; usual maximum is ~75 mg, but additional carbidopa (Lodosyn) 25 mg can be added for persistent nausea. (Katzung 16e Ch.28, p.520)
- Combination name — Co-careldopa. (KDT 8e Ch.31, p.457)
- Indian preparations — TIDOMET-LS, SYNDOPA-110, SINEMET, DUODOPA-110: 10 mg + 100 mg; TIDOMET PLUS, SYNDOPA PLUS: 25 mg + 100 mg; TIDOMET FORTE, SYNDOPA-275: 25 mg + 250 mg; BENSPAR, MADOPAR: benserazide 25 mg + levodopa 100 mg. (KDT 8e Ch.31, p.457)
- Maintenance — levodopa 0.4–0.8 g/day with 75–100 mg carbidopa or 100–200 mg benserazide, in 3–4 divided doses. (KDT 8e Ch.31, p.457)
- Initiation regimen (Katzung) — carbidopa 25 mg + levodopa 100 mg TID, 30–60 min before meals; titrate to typical maintenance 25/250 TDS or QID. (Katzung 16e Ch.28, p.520)
14. Newer levodopa formulations
- Sinemet CR — older sustained-release in erodable wax matrix; useful for fluctuations and reduced dosing frequency, but absorption unpredictable. (Katzung 16e Ch.28, p.520)
- Rytary (extended-release CD/LD) — capsules with beads releasing CD/LD in 1:4 ratio at different rates over a prolonged period; substituted for IR using manufacturer dose-conversion table. (Katzung 16e Ch.28, p.520)
- Rytary conversion examples — 400–549 mg total daily IR levodopa → 23.75/95, 3 caps TID; 750–949 → 36.25/145, 3 caps TID; ≥1250 → 48.75/195, 4 caps TID or 61.25/245, 3 caps TID. (Katzung 16e Ch.28, p.520)
- Parcopa (10/100, 25/100, 25/250) — orally disintegrating CD/LD; ~1 h before meals; Katzung notes Parcopa was discontinued in the US. (Katzung 16e Ch.28, p.520; G&G 14e Ch.21, p.424)
- Stalevo — triple combination LD + CD + entacapone in three strengths: 50 (50/12.5/200), 100 (100/25/200), 150 (150/37.5/200); simplifies regimen but earlier and ↑ frequency of dyskinesia compared with CD/LD alone. (Katzung 16e Ch.28, p.526)
- Duodopa / Duopa intestinal gel — continuous CD/LD via percutaneous endoscopic gastrostomy with jejunal extension; morning bolus 100–300 mg LD then continuous 40–120 mg/h with supplemental boluses; superior to oral in advanced PD with response fluctuations. (Katzung 16e Ch.28, p.520)
- Inbrija (inhaled levodopa powder) — intermittent treatment of off-periods. (Katzung 16e Ch.28, p.522)
- Subcutaneous levodopa — delivery is in development, now realised as subcutaneous foslevodopa-foscarbidopa (see Recent Advances). (G&G 14e Ch.21, p.417)
15. DA agonists — general principles
- Advantage 1 — act directly on postsynaptic striatal DA receptors — independent of surviving presynaptic neurones; effective even in advanced disease with loss of synthetic/storage capacity. (KDT 8e Ch.31, p.457; Katzung 16e Ch.28, p.523)
- Advantage 2 — longer duration of action than levodopa. (KDT 8e Ch.31, p.457)
- Advantage 3 — can be subtype-selective (D2/D3). (KDT 8e Ch.31, p.457)
- Advantage 4 — no oxidative metabolism to potentially neurotoxic intermediates → theoretical neuroprotection. (KDT 8e Ch.31, p.457)
- Advantage 5 — no competition with dietary amino acids for transport. (KDT 8e Ch.31, p.457)
- vs Levodopa — efficacy — less symptomatic benefit than levodopa. (Katzung 16e Ch.28, p.523)
- vs Levodopa — fluctuations — lower incidence of dyskinesias and motor fluctuations when used as initial therapy (PD MED trial). (KDT 8e Ch.31, p.458; G&G 14e Ch.21, p.418)
- vs Levodopa — AEs — higher incidence of mental side effects, somnolence, edema, and impulse-control disorders. (Katzung 16e Ch.28, p.523; G&G 14e Ch.21, p.418)
- First-line role — younger patients with mild PD (avoid if age >70 or if ICD risk factors). (Katzung 16e Ch.28, p.529)
- Adjunct role — in advanced PD with end-of-dose akinesia or on–off; usually requires lowering levodopa dose. (Katzung 16e Ch.28, p.523)
- No-response caveat — disappointing response if patient has never responded to levodopa. (Katzung 16e Ch.28, p.523)
16. Bromocriptine
- Profile — ergot derivative; potent D2 agonist, partial agonist or antagonist at D1. (KDT 8e Ch.31, p.457)
- Onset / duration — onset ½–1 h after oral; duration 6–10 h. (KDT 8e Ch.31, p.457)
- Largely replaced — by ropinirole/pramipexole due to high incidence of intolerable AEs: vomiting, hallucinations, hypotension, nasal stuffiness, conjunctival injection. (KDT 8e Ch.31, p.457)
- First-dose hypotension — marked, especially in patients on antihypertensives. (KDT 8e Ch.31, p.457)
- Dose — 1.25 mg ON, increase up to 5 mg TDS. (KDT 8e Ch.31, p.457)
- Indian brands — PROCTINAL, SICRIPTIN, PARLODEL 1.25/2.5 mg; ENCRIPT 2.5/5 mg. (KDT 8e Ch.31, p.457)
17. Pergolide
- Profile — ergot derivative; D1 + D2 agonist. (Katzung 16e Ch.28, p.524)
- Status — withdrawn from US market due to association with valvular heart disease; still available in some countries. (Katzung 16e Ch.28, p.524)
18. Pramipexole
- Profile — non-ergoline; selective D2/D3 agonist with relatively greater D3 affinity; negligible D1 or non-dopaminergic affinity. (KDT 8e Ch.31, p.457)
- Putative neuroprotection — scavenges H2O2 and enhances neurotrophic activity in mesencephalic DA cell cultures in vitro. (Katzung 16e Ch.28, p.524)
- Mood — possible mood-elevating effect — may ameliorate affective symptoms. (Katzung 16e Ch.28, p.524)
- PK — rapidly absorbed orally; Tmax ~2 h; excreted largely unchanged in urine → dose adjustment in renal insufficiency. (Katzung 16e Ch.28, p.524)
- Dosing (Katzung) — start 0.125 mg TDS; double after 1 week, then again after another week; further weekly 0.75 mg/day increments; most patients require 0.5–1.5 mg TDS. (Katzung 16e Ch.28, p.524)
- Dosing (KDT) — titrate from 0.125 mg TDS to 0.5–1.5 mg TDS. (KDT 8e Ch.31, p.458)
- Potency — twice as potent as ropinirole but comparable in efficacy and tolerability. (KDT 8e Ch.31, p.458)
- ER preparation — extended-release once-daily — same total daily dose, smoother levels. (Katzung 16e Ch.28, p.524)
- Indian brands — PRAMIPEX 0.125/0.25/0.5/1 mg; PARPEX 0.5/1.0/1.5 mg; PRAMIROL 0.125/0.25/0.5/1.0/1.5 mg. (KDT 8e Ch.31, p.458)
19. Ropinirole
- Profile — non-ergoline; relatively pure D2 agonist with negligible D1 activity. (KDT 8e Ch.31, p.458; Katzung 16e Ch.28, p.524)
- PK — rapidly absorbed; 40 % plasma protein bound; extensively metabolised by hepatic CYP1A2 to inactive metabolites; terminal t½ ~6 h — longer-acting than levodopa. (KDT 8e Ch.31, p.458)
- CYP1A2 interaction — drugs metabolised by 1A2 (e.g. ciprofloxacin) ↑ ropinirole levels; smoking induces 1A2. (Katzung 16e Ch.28, p.524)
- Dosing — start 0.25 mg TDS; total daily dose ↑ by 0.75 mg weekly to week 4, then by 1.5 mg/week; most patients 2–8 mg TDS; max 8 mg TDS. (KDT 8e Ch.31, p.458; Katzung 16e Ch.28, p.524)
- Early disease — 1–2 mg TDS generally adequate. (KDT 8e Ch.31, p.458)
- Prolonged-release — once-daily preparation available. (Katzung 16e Ch.28, p.524)
- Other indication — FDA-approved for restless legs syndrome. (KDT 8e Ch.31, p.458)
- Indian brands — ROPITOR, ROPARK, ROPIN, ROPEWAY 0.25/0.5/1.0/2.0 mg. (KDT 8e Ch.31, p.458)
20. Rotigotine
- Profile — non-ergot D2/D1 agonist via transdermal patch for continuous 24-h dopaminergic stimulation. (Katzung 16e Ch.28, p.524)
- Theoretical advantage — reduces pulsatile-stimulation-driven dyskinesia. (Katzung 16e Ch.28, p.524)
- Dosing — start 2 mg/24 h patch; titrate weekly to 4 mg/24 h then 6 mg/24 h. (Katzung 16e Ch.28, p.524)
- Indication — approved for early PD; efficacy in advanced disease less clear. (Katzung 16e Ch.28, p.524)
- Application-site — reactions can be serious. (Katzung 16e Ch.28, p.524)
- Other indication — RLS.
21. Apomorphine
- Profile — non-ergoline potent agonist; high D4 affinity; moderate at D2/D3/D5 + α1D, α2B, α2C; low D1 affinity. (Katzung 16e Ch.28, p.526)
- Indication — rescue therapy for acute intermittent treatment of off-periods in patients on optimised dopaminergic therapy. (Katzung 16e Ch.28, p.526)
- Onset / duration — within ~10 min of subcutaneous injection; duration up to 2 h. (Katzung 16e Ch.28, p.526)
- Antiemetic premed — highly emetogenic — requires trimethobenzamide 300 mg TDS for 3 days before initiation, continued ≥1 month. (Katzung 16e Ch.28, p.526)
- Critical interaction — contraindicated with 5-HT3 antagonists (e.g. ondansetron) — risk of profound hypotension and loss of consciousness. (Katzung 16e Ch.28, p.526)
- Dosing — test dose 2 mg SC under supine + standing BP monitoring; titrate to 3–6 mg per dose; usual ≤3 doses/day (max 5); also continuous infusion. (Katzung 16e Ch.28, p.526)
- Sublingual film — 10 mg starting; titrate to max 30 mg/dose, up to 5 doses/day; can cause oral ulcers. (G&G 14e Ch.21, p.418)
- AEs — dyskinesias, drowsiness, insomnia, chest pain, sweating, hypotension, syncope, constipation, panniculitis, injection-site bruising; QT prolongation. (Katzung 16e Ch.28, p.526)
22. DA agonists — adverse effects (class)
- GI — anorexia, nausea, vomiting (minimised by taking with meals); constipation, dyspepsia, reflux; rarely peptic-ulcer bleeding. (Katzung 16e Ch.28, p.524)
- Cardiovascular — postural hypotension at initiation; painless digital vasospasm (dose-related, ergot-derivatives); peripheral oedema; cardiac arrhythmias warrant discontinuation; valvulopathy with pergolide. (Katzung 16e Ch.28, p.524)
- Dyskinesias — similar to levodopa-induced; reverse with dose reduction. (Katzung 16e Ch.28, p.524)
- Mental disturbances — confusion, hallucinations, delusions; more common and severe than with levodopa; tend to occur earlier in older patients; respond to atypical antipsychotics or pimavanserin. (Katzung 16e Ch.28, p.524)
- ICDs — definition — compulsive gambling, shopping, betting, sexual behaviour, eating; prevalence up to 45 % of PD patients on DA agonists. (Katzung 16e Ch.28, p.525)
- ICDs — mechanism — activation of D2/D3 receptors in mesocorticolimbic system. (Katzung 16e Ch.28, p.525)
- ICDs — dynamics — dose- and duration-related; idiosyncratic between agents; resolve on withdrawal. (Katzung 16e Ch.28, p.525)
- ICDs — risk factors — impulsive personality, prior addictive behaviours, family history of gambling. (Katzung 16e Ch.28, p.525)
- ICDs — screening — generally under-reported by patients; active screening is essential; higher rate with DA agonists than levodopa. (G&G 14e Ch.21, p.418)
- Sleep attacks — sudden-onset sleep documented with both ropinirole and pramipexole; advise patients not to drive if affected. (KDT 8e Ch.31, p.458)
- DAWS — DA agonist withdrawal syndrome — anxiety, agitation, panic, depression, suicidal ideation, irritability, fatigue, postural hypotension, nausea, vomiting, diaphoresis, drug cravings. (Katzung 16e Ch.28, p.525)
- DAWS — features — refractory to levodopa and other dopaminergics; may persist months; risk factors prior ICDs and higher cumulative agonist dose. (Katzung 16e Ch.28, p.525)
- DAWS — management — no effective treatment — slow taper or reintroduction with gradual taper. (Katzung 16e Ch.28, p.525)
- Misc — headache, nasal congestion, increased arousal, pulmonary infiltrates/pleural and retroperitoneal fibrosis (ergot-derivatives), erythromelalgia (red, painful, swollen feet ± hands; clears days after withdrawal). (Katzung 16e Ch.28, p.525)
23. DA agonists — contraindications
- Avoid in — psychotic illness, recent MI, active peptic ulcer. (Katzung 16e Ch.28, p.525)
- Ergot-derived — avoid in peripheral vascular disease. (Katzung 16e Ch.28, p.525)
- Withdrawal caution — do not stop abruptly — may rarely lead to akinetic crisis or NMS-like syndrome. (Katzung 16e Ch.28, p.525)
24. MAO isoforms — basis for selectivity
- Two isoenzymes — MAO-A (prefers serotonin, NA) and MAO-B (prefers DA in CNS); both metabolise DA peripherally. (KDT 8e Ch.31, p.458; Katzung 16e Ch.28, p.525)
- MAO-B distribution — predominates in the brain and platelets. (KDT 8e Ch.31, p.458)
- Cheese reaction — selective MAO-B inhibitors at therapeutic doses do NOT cause it because peripheral metabolism of dietary tyramine is preserved by intact MAO-A. (Katzung 16e Ch.28, p.525; KDT 8e Ch.31, p.458)
- Loss of selectivity — at higher doses, selegiline loses MAO-B selectivity and can inhibit MAO-A → potential hypertensive interaction. (Katzung 16e Ch.28, p.525)
25. Selegiline (Deprenyl, l-deprenyl)
- Profile — selective irreversible MAO-B inhibitor at low doses (≤10 mg/day). (KDT 8e Ch.31, p.458)
- Mechanism in PD — ↓ intracerebral DA degradation → ↑ striatal DA availability. (KDT 8e Ch.31, p.458)
- Monotherapy — mild antiparkinsonian action alone in early/mild PD. (KDT 8e Ch.31, p.458)
- As adjuvant 1 — prolongs and enhances levodopa action. (KDT 8e Ch.31, p.458)
- As adjuvant 2 — attenuates motor fluctuations, ↓ wearing-off. (KDT 8e Ch.31, p.458)
- As adjuvant 3 — beneficial in 50–70 % of patients; permits 20–30 % reduction in levodopa dose. (KDT 8e Ch.31, p.458)
- Limitations — advanced cases with on–off effect not improved; peak-dose AEs (dyskinesia, confusion, hallucinations) may be worsened; clinical benefit short-lived (6–26 months). (KDT 8e Ch.31, p.458)
- Putative neuroprotection (DATATOP) — based on idea that MAO-B oxidises DA/MPTP-like toxins → free radicals → nigrostriatal damage; large trials have NOT detected a difference in disease progression with selegiline; recent rasagiline data more promising. (KDT 8e Ch.31, p.459)
- Metabolites — metabolised by liver to L-amphetamine and L-methamphetamine → may cause insomnia, agitation, anxiety; advise to take in morning/lunch only. (KDT 8e Ch.31, p.459; Katzung 16e Ch.28, p.525)
- Dose — 5 mg with breakfast + 5 mg with lunch; reduce levodopa by ¼ after 2–3 days of adding selegiline. (KDT 8e Ch.31, p.459)
- Indian brands — ELDEPRYL 5/10 mg; SELERIN, SELGIN 5 mg. (KDT 8e Ch.31, p.459)
- Other formulations — orally disintegrating tablet and transdermal patch (Emsam) — both reduce hepatic first-pass and amphetamine-metabolite formation. (G&G 14e Ch.21, p.419)
- Contraindication — convulsive disorders. (KDT 8e Ch.31, p.459)
- Pethidine interaction — favours metabolism to norpethidine → excitement, rigidity, hyperthermia, respiratory depression. (KDT 8e Ch.31, p.459)
- Other interactions — avoid tramadol, methadone, propoxyphene, dextromethorphan, cyclobenzaprine, St John's wort, TCAs, SSRIs. (KDT 8e Ch.31, p.459; G&G 14e Ch.21, p.419)
- Serotonin syndrome — theoretical risk with antidepressants — rare in practice; if needed, low-dose antidepressant + close monitoring. (Katzung 16e Ch.28, p.525)
26. Rasagiline
- Profile — newer selective irreversible MAO-B inhibitor with selegiline-like action. (KDT 8e Ch.31, p.459)
- Advantage 1 — 5× more potent than selegiline. (KDT 8e Ch.31, p.459)
- Advantage 2 — longer-acting; once-daily morning dose. (KDT 8e Ch.31, p.459)
- Advantage 3 — NOT metabolised to amphetamine → no excitatory side effects or insomnia. (KDT 8e Ch.31, p.459)
- Preferred status — now preferred over selegiline. (KDT 8e Ch.31, p.459)
- Indications — monotherapy in early PD; adjunctive 0.5–1 mg/day for motor fluctuations. (Katzung 16e Ch.28, p.525)
- Possible neuroprotection (ADAGIO) — delayed-start design — 1 mg/day met all endpoints suggesting disease modification, but 2 mg/day did not — results difficult to interpret; decision is individualised. (Katzung 16e Ch.28, p.525)
- Dose — 1 mg OD in morning. (KDT 8e Ch.31, p.459)
- Indian brands — RELGIN, RASALECT 0.5/1.0 mg; RASIPAR 1 mg. (KDT 8e Ch.31, p.459)
27. Safinamide
- Profile — third MAO-B inhibitor; reversible (unlike selegiline/rasagiline). (Katzung 16e Ch.28, p.525)
- Additional mechanism — inhibits glutamate release — possible advantage for dyskinesia. (G&G 14e Ch.21, p.419)
- Adjunctive only — not effective as monotherapy. (Katzung 16e Ch.28, p.525)
- Use — to reduce off-periods in patients with wearing-off or on–off. (Katzung 16e Ch.28, p.525)
- Dose — 50 mg OD initially, ↑ to 100 mg OD after 2 weeks. (Katzung 16e Ch.28, p.525)
- Hepatic — avoid in severe impairment; dose-adjust in moderate. (G&G 14e Ch.21, p.419)
- Interactions — same drug-interaction profile as selegiline/rasagiline. (G&G 14e Ch.21, p.419)
28. COMT inhibitors — rationale
- Rationale — when peripheral DDC is blocked by carbidopa, levodopa is preferentially metabolised by COMT to 3-OMD. (KDT 8e Ch.31, p.459)
- Effect of COMT block — prolongs levodopa t½, ↓ levodopa clearance, ↑ relative bioavailability. (Katzung 16e Ch.28, p.526)
- What does NOT change — peak levodopa concentration and time-to-peak — only duration of effect. (Katzung 16e Ch.28, p.526)
- 3-OMD effect — competes with levodopa for active BBB transport — lowering 3-OMD itself improves levodopa entry. (KDT 8e Ch.31, p.459)
- Central COMT — in brain also degrades DA — central COMT inhibition could preserve striatal DA. (KDT 8e Ch.31, p.459)
- Indication — adjunct to LD/CD in advanced PD with motor fluctuations to ↓ wearing-off, ↑ on-time, ↓ off-time, allow LD dose reduction. (KDT 8e Ch.31, p.459)
- Not for — early/initial therapy. (Katzung 16e Ch.28, p.526)
29. Entacapone
- Profile — reversible, peripheral-only COMT inhibitor (short t½ ~2 h limits central penetration). (KDT 8e Ch.31, p.459)
- Dose — 200 mg with each LD/CD dose, max 1600 mg/day. (KDT 8e Ch.31, p.459)
- Indian brands — ADCAPON, COMTAN 200 mg. (KDT 8e Ch.31, p.459)
- Triple combination — available as Stalevo (LD + CD + entacapone). (Katzung 16e Ch.28, p.526)
- Hepatotoxicity — not hepatotoxic. (KDT 8e Ch.31, p.459)
- Preferred — generally over tolcapone. (Katzung 16e Ch.28, p.526)
30. Tolcapone
- Profile — reversible COMT inhibitor with central + peripheral action; longer-acting, slightly more potent than entacapone. (Katzung 16e Ch.28, p.526)
- Dose — 100 mg BD or TDS, up to 200 mg TDS. (KDT 8e Ch.31, p.459)
- Black-box hepatotoxicity — acute fatal hepatitis and rhabdomyolysis reported → suspended in Europe and Canada; in USA only with informed consent for entacapone non-responders + LFT monitoring every 2–4 weeks for 6 months, then periodically. (KDT 8e Ch.31, p.459; Katzung 16e Ch.28, p.526)
- Withdrawal rule — withdraw and do not reintroduce if hepatic injury develops. (Katzung 16e Ch.28, p.526)
31. Opicapone
- Profile — newer long-acting, peripheral-only COMT inhibitor. (Katzung 16e Ch.28, p.526)
- Dosing — once-daily 50 mg at bedtime despite short plasma t½ — slow dissociation rate. (Katzung 16e Ch.28, p.526)
- Efficacy — ↓ daily off-time and ↑ on-time, comparable to entacapone. (G&G 14e Ch.21, p.418)
- Brand — Ongentys. (Katzung 16e Ch.28, p.526)
32. COMT inhibitors — adverse effects
- Class AEs — mostly reflect ↑ levodopa exposure: dyskinesias, nausea, vomiting, postural hypotension, hallucinations, confusion. (KDT 8e Ch.31, p.459)
- Levodopa dose — lower by 20–30 % in first 48 h to avoid these. (KDT 8e Ch.31, p.459; Katzung 16e Ch.28, p.526)
- Diarrhoea — 10–18 % (less with entacapone); may be delayed by weeks–months. (KDT 8e Ch.31, p.459)
- Urine — yellow-orange discoloration — harmless. (KDT 8e Ch.31, p.460)
- Other — sleep disturbance, abdominal pain. (Katzung 16e Ch.28, p.526)
- Tolcapone-specific — ↑ liver enzymes, fatal hepatotoxicity. (Katzung 16e Ch.28, p.526)
- Stalevo — earlier onset and ↑ frequency of dyskinesia compared with CD/LD alone; no increased CV risk demonstrated despite earlier concern. (Katzung 16e Ch.28, p.526)
33. Amantadine
- Origin — originally developed as antiviral for influenza A2; antiparkinsonian effect discovered serendipitously. (KDT 8e Ch.31, p.459)
- Mechanism — multi-modal — promotes presynaptic synthesis and release of DA; NMDA-glutamate-receptor antagonism (basis of antidyskinetic action); anticholinergic; releases catecholamines from peripheral stores; antagonises adenosine A2A receptors → may potentiate D2 signalling. (KDT 8e Ch.31, p.460; Katzung 16e Ch.28, p.527; G&G 14e Ch.21, p.419)
- Efficacy — lower than levodopa, comparable to anticholinergics; ~⅔ of patients derive some benefit; tolerance develops over weeks to months. (KDT 8e Ch.31, p.460)
- Clinical role 1 — mild early disease (monotherapy). (KDT 8e Ch.31, p.460)
- Clinical role 2 (key niche) — suppression of levodopa-induced dyskinesias and motor fluctuations in advanced disease. (KDT 8e Ch.31, p.460; Katzung 16e Ch.28, p.527)
- Dose — 100 mg BD (fixed; not titrated); single-dose effect lasts 8–12 h. (KDT 8e Ch.31, p.460)
- Symmetrel (IR) — 100 mg BD or TDS. (Katzung 16e Ch.28, p.527)
- Gocovri — ER once daily at bedtime. (Katzung 16e Ch.28, p.527)
- Osmolex — 129–322 mg ER once daily in morning. (Katzung 16e Ch.28, p.527)
- PK — peak 1–4 h; t½ 2–4 h; mostly excreted unchanged in urine — caution in renal impairment. (Katzung 16e Ch.28, p.527)
- Indian brand — AMANTREL, COMANTREL 100 mg. (KDT 8e Ch.31, p.460)
- AEs — CNS — insomnia, restlessness, confusion, nightmares, hallucinations (rare), depression, suicidal ideation, irritability, ICDs, agitation, excitement, psychosis, convulsions at high doses. (KDT 8e Ch.31, p.460; Katzung 16e Ch.28, p.527)
- Livedo reticularis — + ankle oedema — characteristic; due to local catecholamine release causing postcapillary vasoconstriction; clears within ~1 month of stopping. (KDT 8e Ch.31, p.460)
- Anticholinergic AEs — dry mouth, urinary retention, blurred vision, constipation. (KDT 8e Ch.31, p.460)
- Other AEs — headache, heart failure, postural hypotension, GI upset. (KDT 8e Ch.31, p.460)
- Cautions — seizure history, heart failure, moderate–severe renal disease. (Katzung 16e Ch.28, p.527)
- Withdrawal — avoid abrupt — acute confusional state, hyperpyrexia, parkinsonism worsening. (Katzung 16e Ch.28, p.527)
- Combination — side effects accentuated when combined with anticholinergics. (KDT 8e Ch.31, p.460)
34. Istradefylline
- Profile — caffeine analogue; selective adenosine A2A receptor antagonist. (Katzung 16e Ch.28, p.527)
- Rationale — A2A receptors are highly co-localised with D2 in striatum; A2A-D2 heterodimers; A2A activation inhibits D2 signalling — so A2A antagonism boosts dopaminergic tone. (G&G 14e Ch.21, p.419)
- Indication — adjunct to LD/CD for off-periods; not effective as monotherapy. (G&G 14e Ch.21, p.419)
- Dose — 20 or 40 mg PO once daily. (Katzung 16e Ch.28, p.527)
- AEs — dyskinesias, dizziness, constipation, nausea, hallucinations, sleeplessness, ICDs. (Katzung 16e Ch.28, p.527)
- Non-motor benefit — possible benefit on urinary dysfunction, daytime sleepiness, cognition — small open-label data only. (G&G 14e Ch.21, p.419)
- Coverage — absent from KDT 8e (predates 2019 FDA approval).
35. Central anticholinergics — overview
- Class profile — drugs with higher central : peripheral anticholinergic action ratio than atropine; pharmacological profile otherwise similar. (KDT 8e Ch.31, p.460)
- Antihistaminic overlap — certain H1 antihistaminics also have significant central anticholinergic property and overlap clinically. (KDT 8e Ch.31, p.460)
- Mechanism — ↓ unbalanced cholinergic activity in striatum (the cholinergic interneurones) — restoring DA/ACh balance. (KDT 8e Ch.31, p.460)
- Site of action — likely the muscarinic receptors mediating cholinergic interneurone effects on striatal projection neurones. (G&G 14e Ch.21, p.419)
- Efficacy — 10–25 % improvement in parkinsonian symptoms after single dose; effect lasts 4–8 hours. (KDT 8e Ch.31, p.460)
- Symptom profile — tremor benefited more than rigidity; hypokinesia improved least. (KDT 8e Ch.31, p.460; Katzung 16e Ch.28, p.527)
- Sialorrhoea — controlled by peripheral antimuscarinic action. (KDT 8e Ch.31, p.460)
- Place 1 — mild cases or when levodopa contraindicated. (KDT 8e Ch.31, p.460)
- Place 2 — combined with levodopa to lower levodopa dose. (KDT 8e Ch.31, p.460)
- Place 3 (key) — drugs of choice for drug-induced (D2-antagonist) parkinsonism — only effective class in this setting. (KDT 8e Ch.31, p.460; Katzung 16e Ch.28, p.529)
- Disadvantage 1 — far less efficacious than levodopa. (KDT 8e Ch.31, p.460)
- Disadvantage 2 — poorly tolerated by elderly (memory and cognition impairment, organic confusional states, blurred vision, urinary retention especially in elderly males). (KDT 8e Ch.31, p.460)
- Antihistaminics — less efficacious but better tolerated by older patients; sedative effect helps in some. (KDT 8e Ch.31, p.460)
- Orphenadrine — has mild euphoriant effect. (KDT 8e Ch.31, p.460)
- Suppurative parotitis — can complicate xerostomia. (Katzung 16e Ch.28, p.527)
- Withdrawal — must be gradual — abrupt cessation may exacerbate parkinsonism. (Katzung 16e Ch.28, p.527)
36. Specific anticholinergic agents
- Most commonly used — trihexyphenidyl — start at lowest dose in 2–3 divided portions, increase till side effects are tolerated. (KDT 8e Ch.31, p.460)
- Katzung daily ranges — benztropine 1–6 mg; biperiden 2–12 mg; orphenadrine 150–400 mg; procyclidine 7.5–30 mg; trihexyphenidyl 6–20 mg. (Katzung 16e Ch.28, p.527)
- Diphenhydramine — also used clinically (50 mg IV) for dystonic reactions and as a mild antiparkinsonian. (G&G 14e Ch.21, p.419)
- Trial of another agent — reasonable if first does not work — individual response variability. (Katzung 16e Ch.28, p.527)
37. Treatment philosophy
- Disease-modifying — none of the available drugs alters the basic pathology — disease continues to progress; drugs provide symptomatic relief and add 5–10 years of better-quality life. (KDT 8e Ch.31, p.460)
- Free-radical concern — levodopa metabolism produces free radicals that may hasten degeneration; controlled prospective studies have not detected such acceleration, but dyskinesia incidence is dose- and duration-related. (KDT 8e Ch.31, p.460)
- Best results — in the first few years of levodopa treatment; daily dose may need reduction over time; benefit declines after 3–4 years regardless of initial response. (Katzung 16e Ch.28, p.520)
- Mortality — early initiation lowers mortality but does not stop progression. (Katzung 16e Ch.28, p.520)
- PD MED 2014 — patients started on levodopa had small but persistent benefit in mobility and ADLs at 7 years vs DA agonists or MAO-B inhibitors, though dyskinesia was higher in the levodopa group. (G&G 14e Ch.21, p.417)
- Delay until symptoms impact lifestyle — many authorities now recommend delaying initiation of dopaminergics until symptoms impact lifestyle. (KDT 8e Ch.31, p.460; G&G 14e Ch.21, p.420)
38. Stepwise approach to PD pharmacotherapy
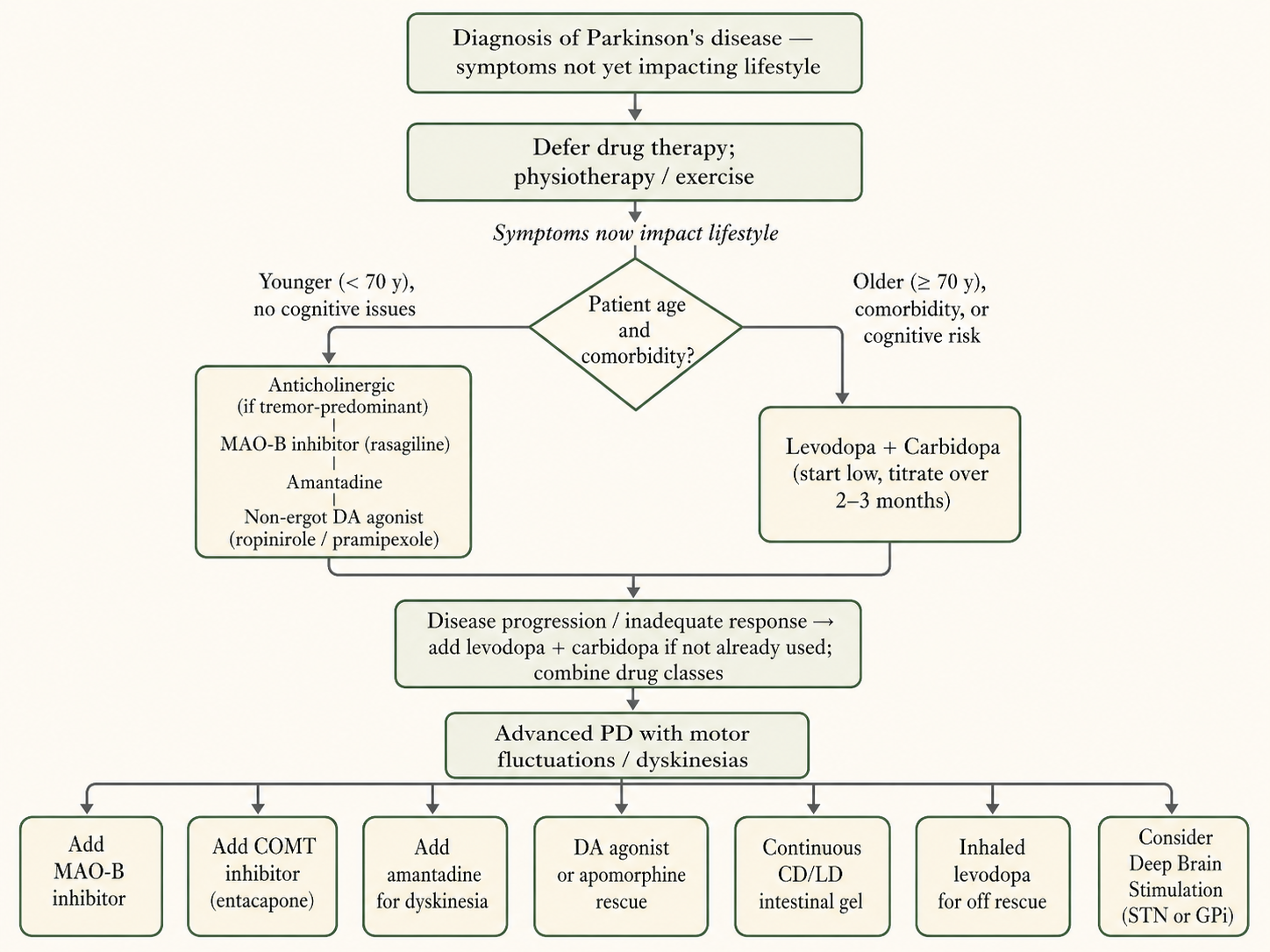
- Step 1 — drug therapy not yet needed — exercise, physiotherapy, education. (G&G 14e Ch.21, p.420)
- Step 2 — mild symptoms requiring drugs — anticholinergics (younger, tremor-predominant); selegiline / rasagiline (possible disease-modifying); amantadine (broad mild benefit); non-ergot DA agonist. (KDT 8e Ch.31, p.460)
- Anticholinergic caveat — often poorly tolerated by elderly (especially men). (KDT 8e Ch.31, p.460)
- Step 3 — younger patients — inadequate response or progression → start with non-ergot DA agonist (ropinirole/pramipexole) monotherapy to delay levodopa. (KDT 8e Ch.31, p.461; Katzung 16e Ch.28, p.529)
- Step 4 — older (>70 y) or comorbid — start LD/CD directly — better tolerated. (Katzung 16e Ch.28, p.529)
- Step 5 — slow titration — of LD/CD over 2–3 months, with frequent evaluation; full benefit lasts ~2–3 years before declining. (KDT 8e Ch.31, p.461)
39. Management of motor fluctuations
- Typical progression — after 4–8 years, wearing-off → dyskinesias → on–off. (KDT 8e Ch.31, p.461)
- Wearing-off — dose fractionation — more frequent smaller LD/CD doses. (KDT 8e Ch.31, p.461)
- Wearing-off — MAO-B — add MAO-B inhibitor (rasagiline preferred) to prolong LD action. (KDT 8e Ch.31, p.461)
- Wearing-off — COMT — add COMT inhibitor entacapone with each LD dose. (KDT 8e Ch.31, p.461)
- Wearing-off — Rytary — switch to extended-release LD/CD. (Katzung 16e Ch.28, p.520)
- Wearing-off — DA agonist — add to smooth on–off. (KDT 8e Ch.31, p.461)
- Apomorphine SC — rescue for off-periods. (Katzung 16e Ch.28, p.526)
- Inhaled levodopa — (Inbrija) for intermittent off-rescue. (Katzung 16e Ch.28, p.522)
- LD/CD intestinal gel — (Duodopa) for advanced refractory cases. (Katzung 16e Ch.28, p.520)
- Dyskinesias — LD reduction — worsens parkinsonism — accept some trade-off.
- Dyskinesias — amantadine — first-line antidyskinetic. (KDT 8e Ch.31, p.460; Katzung 16e Ch.28, p.522)
- Dyskinesias — clozapine — second-line option. (Katzung 16e Ch.28, p.522)
- Dyskinesias — continuous delivery — intrajejunal LD, transdermal rotigotine. (Katzung 16e Ch.28, p.522)
- Dietary protein redistribution — main protein meal in evening can ↓ daytime fluctuations. (Katzung 16e Ch.28, p.522)
- Drug holiday — no longer practiced. (KDT 8e Ch.31, p.461)
40. Surgical procedures
- DBS — ablative lesions (pallidotomy, thalamotomy) largely replaced by deep brain stimulation with implanted electrode + stimulator — lower morbidity, reversible, adjustable. (Katzung 16e Ch.28, p.527)
- DBS targets — subthalamic nucleus (STN) — most common; globus pallidus interna (GPi). (Katzung 16e Ch.28, p.527)
- Indications — moderate PD with motor fluctuations or dyskinesias inadequately controlled with medication. (Katzung 16e Ch.28, p.527)
- Contraindications — secondary or atypical parkinsonism, dementia, failure to respond to dopaminergic medication. (Katzung 16e Ch.28, p.527)
- Medication post-DBS — antiparkinsonian medication can often be reduced post-DBS, ameliorating dose-related AEs. (Katzung 16e Ch.28, p.527)
- MRgFUS — magnetic-resonance-guided focused ultrasound thalamotomy — option for medication-refractory tremor-predominant PD in patients unwilling to undergo DBS. (Katzung 16e Ch.28, p.528)
41. Therapy for non-motor symptoms
- Cognitive decline — rivastigmine 1.5–6 mg BD; memantine 5–10 mg/day; donepezil 5–10 mg/day. (Katzung 16e Ch.28, p.528)
- Affective disorders — SSRIs / SNRIs / anxiolytics. (Katzung 16e Ch.28, p.528)
- Psychosis / hallucinations — atypical antipsychotics (clozapine, quetiapine) or pimavanserin. (Katzung 16e Ch.28, p.528)
- Excessive daytime sleepiness — modafinil 100–400 mg morning. (Katzung 16e Ch.28, p.528)
- Bladder/bowel dysfunction — symptomatic therapy. (Katzung 16e Ch.28, p.528)
- REM-sleep behaviour disorder — clonazepam, melatonin (clinical practice).
42. Atypical parkinsonism
- Distinguishing features — inconspicuous tremor, symmetry, additional findings: dysautonomia, cerebellar deficits, eye-movement abnormalities, early cognitive/behavioural changes. (Katzung 16e Ch.28, p.529)
- MSA — multisystem atrophy — autonomic failure + parkinsonism / cerebellar features. (Katzung 16e Ch.28, p.529)
- PSP — progressive supranuclear palsy — vertical gaze palsy, early postural instability, falls. (Katzung 16e Ch.28, p.529)
- CBD — corticobasal degeneration — markedly asymmetric parkinsonism, alien limb, apraxia. (Katzung 16e Ch.28, p.529)
- DLB — diffuse Lewy body disease — early dementia + visual hallucinations. (Katzung 16e Ch.28, p.529)
- Prognosis — worse than PD; response to antiparkinsonian treatment limited; treatment is symptomatic. (Katzung 16e Ch.28, p.529)
43. Drug-induced parkinsonism
- DA depleters — reserpine, tetrabenazine, deutetrabenazine, valbenazine (VMAT2 blockers). (Katzung 16e Ch.28, p.529)
- DA receptor blockers — haloperidol, phenothiazines, metoclopramide. (Katzung 16e Ch.28, p.529)
- Onset — typically within 3–4 months of drug introduction; tends to be symmetric with inconspicuous tremor. (Katzung 16e Ch.28, p.529)
- Course — dose-related; clears over weeks to months after withdrawal. (Katzung 16e Ch.28, p.529)
- Treatment — stop offending drug if possible; anticholinergics preferred if treatment is needed; levodopa is unhelpful while neuroleptics continue and may aggravate underlying psychotic illness. (Katzung 16e Ch.28, p.529)
44. Future / disease-modifying therapies
- α-Synuclein mAb — monoclonal antibodies in phase II clinical studies. (G&G 14e Ch.21, p.419)
- LRRK2 inhibitors — in clinical trials. (G&G 14e Ch.21, p.419)
- GBA-pathway therapies — promote β-glucocerebrosidase activity or reduce its substrate. (G&G 14e Ch.21, p.419)
- Active and passive immunisation — against α-synuclein or α-synuclein-mimicking peptide — generally well-tolerated, generates antibodies. (Katzung 16e Ch.28, p.528)
- Failed neuroprotection candidates — coenzyme Q10, creatine, pramipexole, pioglitazone, inosine, isradipine. (Katzung 16e Ch.28, p.528)
- Currently studied — deferiprone (iron chelator), exenatide (GLP-1 agonist). (Katzung 16e Ch.28, p.528)
- Gene therapy — GAD — AAV2-GAD to subthalamic nucleus (↓ STN drive via ↑ GABA synthesis). (Katzung 16e Ch.28, p.528)
- Gene therapy — AADC — AAV2-AADC to putamen (↑ peripheral LD → DA conversion). (Katzung 16e Ch.28, p.528)
- Gene therapy — Neurturin — AAV2-Neurturin to putamen (neurotrophic; disappointing results). (Katzung 16e Ch.28, p.528)
- ProSavin — lentiviral delivery of TH + AADC + GTP-cyclohydrolase 1 to striatum. (Katzung 16e Ch.28, p.528)
45. Restless legs syndrome — clinical features & diagnosis
- Definition — sensorimotor disorder affecting the legs (occasionally arms) during periods of relaxation — irresistible urge to move associated with tingling, itching, discomfort, aching, or cramps; relieved by walking. (KDT 8e Ch.31, p.458; Katzung 16e Ch.28, p.533)
- Sleep impact — may delay sleep onset; associated periodic limb movements of sleep (PLMS) can fragment sleep → daytime sleepiness. (Katzung 16e Ch.28, p.533)
- Aetiology — primary (idiopathic) or secondary to: iron-deficiency anaemia / low ferritin, folate or vitamin deficiencies, varicose veins, peripheral neuropathy, pregnancy. (KDT 8e Ch.31, p.458; Katzung 16e Ch.28, p.533)
- Pathophysiology — mild dopaminergic hypofunction + genetic basis. (KDT 8e Ch.31, p.458)
46. RLS — pharmacological management
- Iron correction — correct ferritin / iron deficiency as primary intervention. (Katzung 16e Ch.28, p.533)
- Avoid exacerbants — serotonergic antidepressants, neuroleptics, metoclopramide, antihistamines, caffeine. (Katzung 16e Ch.28, p.533)
- Drugs of choice — non-ergot DA agonists 2–3 h before bedtime — ropinirole 0.25–4.0 mg; pramipexole 0.125–0.75 mg; rotigotine patch. (Katzung 16e Ch.28, p.533)
- Augmentation — earlier symptom onset, briefer drug response — key complication, especially with LD/CD; switch to a DA agonist if it occurs. (Katzung 16e Ch.28, p.533)
- Alpha-2-delta ligands — gabapentin 300–1800 mg; gabapentin enacarbil 600 or 1200 mg OD; pregabalin 150–300 mg. (Katzung 16e Ch.28, p.533)
- Clonazepam — 1 mg/day for intermittent symptoms. (Katzung 16e Ch.28, p.533)
- Opiates — long t½, low addictive potential — oxycodone when refractory. (Katzung 16e Ch.28, p.533)
Comparison — Levodopa vs DA agonists vs MAO-B inhibitors as initial therapy
RECENT ADVANCES
Recent Advances current as of 09 May 2026
RA 1. New Approvals & Label Expansions
![Figure 9 [RA] — Three modes of continuous-delivery levodopa: oral IR vs LCIG vs Vyalev](images/antiparkinsonian-drugs/pharma_parkinsons-disease_ra_01_foslevodopa-foscarbidopa-subcutaneous-pump.png)
RA 2. Label Changes & Safety Signals
RA 3. Landmark Trials & Meta-Analyses
![Figure 10 [RA] — Major disease-modifying / advanced-PD pivotal trials, 2020–2026](images/antiparkinsonian-drugs/pharma_parkinsons-disease_ra_05_disease-modifying-trials-timeline.png.png)
![Figure 11 [RA] — Disease-modifying therapy targets in Parkinson's disease (2024–2025)](images/antiparkinsonian-drugs/pharma_parkinsons-disease_ra_02_disease-modifying-targets-landscape.png.png)
![Figure 12 [RA] — Tavapadon's selective D₁/D₅ partial agonism vs traditional D₂/D₃ agonist mechanism](images/antiparkinsonian-drugs/pharma_parkinsons-disease_ra_03_tavapadon-d1-selective-mechanism.png.png)
RA 4. Combination Therapies
RA 5. Major Guideline Updates
![Figure 13 [RA] — Updated stepwise treatment algorithm for PD incorporating 2024–2025 advances](images/antiparkinsonian-drugs/pharma_parkinsons-disease_ra_04_updated-treatment-algorithm-2025.png.png)
RA 6. Indian Regulatory & Society Actions
RA 1. New Approvals & Label Expansions
- Foslevodopa–foscarbidopa (Vyalev / Produodopa, AbbVie) — FDA approval 17 Oct 2024 as the first and only subcutaneous 24-hour continuous infusion of a levodopa-based therapy for motor fluctuations in adults with advanced PD. Aqueous prodrugs of carbidopa and levodopa, delivered via the Vyafuser pump; non-surgical alternative to LD/CD intestinal gel (Duodopa). [FDA 2024-Oct]
- Levodopa inhalation powder (Inbrija, Acorda) retains its niche for intermittent off-rescue; label update emphasises that Inbrija is adjunctive to a baseline LD/CD regimen and not for use as primary therapy. [FDA label 2025]
- Pimavanserin (Nuplazid) label remains unchanged for PD psychosis at 34 mg/day, but the FDA boxed-warning prohibition on use in dementia-related psychosis is unchanged after the 3-year post-marketing safety surveillance completed in 2024 — no new mortality signal in the PD-only population. [FDA 2024]
- Opicapone (Ongentys, Neurocrine/BIAL) — once-daily peripheral COMT inhibitor approval extended into multiple Asian markets (2024–2025); not yet CDSCO-approved in India.
RA 2. Label Changes & Safety Signals
- Apomorphine sublingual film (Kynmobi) — manufacturer (Sumitomo) discontinued US distribution in 2024; subcutaneous apomorphine injection (Apokyn) and subcutaneous infusion remain available. Important practical change in off-period rescue armamentarium. [FDA 2024]
- DA agonist withdrawal syndrome (DAWS) — recent prospective cohort and pharmacovigilance data confirm DAWS occurs in 8–19 % of patients tapering pramipexole or ropinirole, with persistence beyond 6 months in a substantial minority; under-reported and lacks effective rescue therapy. [PMID 37147135]
- Levodopa-equivalent daily dose (LEDD) conversion factors updated (Schade et al, Mov Disord 2023): replaces the 2010 Tomlinson formulae with revised conversion ratios for opicapone, safinamide, and istradefylline; relevant for clinical-trial benchmarking and audit work. [PMID 37147135]
- Resting-state fMRI motor network connectivity — emerging biomarker for predicting individual L-dopa responsiveness; not yet ready for clinical use. [PMID 41673341]
RA 3. Landmark Trials & Meta-Analyses
- ELLDOPA (Parkinson Study Group, NEJM 2004) — always-include landmark: placebo-controlled, dose-ranging trial of LD/CD (150–600 mg/d) in 361 early PD patients; clinical benefit was dose-dependent and the 2-week wash-out failed to return motor scores to baseline, suggesting either disease-modifying effect or prolonged pharmacodynamic carry-over; widely cited as the foundational trial against which delayed-start designs are benchmarked.
- PD MED (Lancet 2014) — always-include landmark: open-label pragmatic UK trial of 1,620 newly-diagnosed PD patients randomised to levodopa, DA agonist, or MAO-B inhibitor as initial therapy; at 7 years, levodopa group had small but persistent advantage in mobility and ADL scores, balanced against higher dyskinesia. Foundation for current "levodopa-first" guidance in older patients.
- LIXIPARK (Meissner, Rascol et al, NEJM 2024) — phase 2: 156 early-PD patients on stable dopaminergic therapy randomised to lixisenatide 20 µg SC daily vs placebo for 12 months; MDS-UPDRS Part III on-medication score change was +0.04 with lixisenatide vs +3.04 with placebo (between-group difference 3.08, 95% CI 0.86–5.30; p = 0.007). First positive disease-modifying signal for a GLP-1 RA in PD; offset by nausea 46 %, vomiting 13 %. [PMID 38598572]
- Exenatide-PD3 (Vijiaratnam, Foltynie et al, Lancet 2025) — phase 3: 194 moderate-PD patients randomised to exenatide 2 mg SC weekly vs placebo for 96 weeks; NEGATIVE result — no significant difference in MDS-UPDRS Part III off-medication score progression. Tempers enthusiasm from earlier phase 2 signals; class effect of GLP-1 RAs in PD remains unproven. [Lancet 2025]
- TEMPO-3 (Cerevel/AbbVie, 2024) — phase 3 adjunctive tavapadon: selective D1/D5 partial agonist, once-daily, in adults with PD on stable levodopa with motor fluctuations. Met primary endpoint: +1.1 h additional ON-time without troublesome dyskinesia vs placebo (1.7 h vs 0.6 h; p < 0.0001). Mechanism distinct from existing D2/D3 agonists, theoretically avoiding ICDs and somnolence. NDA filed 2026. [AbbVie press release 2024-Apr]
- TEMPO-1 / TEMPO-2 (AbbVie, 2024) — phase 3 monotherapy tavapadon: in early PD, fixed-dose 5 mg and 15 mg both reduced MDS-UPDRS II + III by ~10 points vs +1.8 with placebo (p < 0.0001 each); flexible-dose TEMPO-2 confirmed monotherapy efficacy. [AbbVie 2024-Sep]
- PASADENA + PADOVA (prasinezumab; Pagano et al, NEJM 2022; Roche 2024 phase 2b PADOVA): humanised anti-aggregated-α-synuclein mAb. PASADENA missed primary endpoint but showed 40–64 % reduction in motor decline in MAO-B-inhibitor subgroup; PADOVA missed the formal primary endpoint but consistent supportive trends. Roche announced phase 3 advance 16 Jun 2025 (n = 900, completion 2029). [Roche 2025-Jun]
- Cinpanemab (Lang et al, NEJM 2022) — phase 2 NEGATIVE: another anti-α-synuclein mAb showed no clinical benefit at any of three doses; reinforces that not all anti-synuclein antibodies behave alike, target engagement and epitope specificity matter. [PMID 35921450]
- FAIRPARK-II (Devos et al, NEJM 2022) — deferiprone phase 2 NEGATIVE/HARMFUL: iron chelator deferiprone 30 mg/kg/d in 372 newly diagnosed PD patients worsened motor function at 36 weeks (between-group difference +2.6 MDS-UPDRS Part III points); definitively closes iron-chelation as a near-term disease-modifying strategy. [PMID 36449420]
- Foslevodopa-foscarbidopa pivotal trial (Soileau et al, Lancet Neurol 2022): 12-week, double-blind, double-dummy, active-controlled phase 3 in 130 advanced-PD patients; subcutaneous foslevodopa-foscarbidopa added +1.79 h ON-time without troublesome dyskinesia and −1.79 h OFF-time vs oral IR LD/CD. Skin-related adverse events and infusion-site reactions are the main tolerability issue. [PMID 36402160]
RA 4. Combination Therapies
- Tavapadon adjunctive to levodopa (TEMPO-3) establishes a new class — D1/D5-selective partial agonist combinations — that may eventually rival D2/D3 agonists as the preferred levodopa-sparing partner, especially in patients at risk of impulse-control disorders.
- Continuous LD/CD delivery (intestinal gel + subcutaneous foslevodopa-foscarbidopa) has matured into a clinically distinct axis of advanced-PD therapy alongside DBS. EAN/MDS-ES 2022 guideline treats device-aided therapy (LCIG, DBS, apomorphine) as the three pillars to be considered in parallel for advanced disease. [EAN/MDS-ES 2022]
- Selegiline/rasagiline + entacapone fixed-dose combinations with low-dose LD/CD — still investigational; aim is to flatten levodopa pharmacokinetics in early disease and delay motor complications.
RA 5. Major Guideline Updates
- AAN Practice Guideline — Dopaminergic therapy for motor symptoms in early PD (Pringsheim et al, Neurology 2021; reaffirmed 8 Feb 2025): levodopa is the preferred initial dopaminergic therapy for motor symptom control in early PD; DA agonists carry higher risk of ICDs, somnolence, edema and hallucinations; MAO-B inhibitors are an option for very mild symptoms with the trade-off of less symptomatic benefit. Risk factors for ICDs explicitly listed: male sex, younger age, history of ICDs, mood disorder, family history of gambling/addiction. [AAN 2021/2025]
- EAN/MDS-ES European section guideline on invasive therapies in PD (Antonini et al, 2022; Brinker et al practical guidance, Mov Disord Clin Pract 2024): defines specific clinical indicators of advanced PD warranting referral for LCIG, DBS, or apomorphine; emphasises early identification rather than reserving these for end-stage disease. [EAN/MDS-ES 2022; Brinker 2024]
- German Society of Neurology (DGN) — Definition and diagnosis of Parkinson's disease (Hopfner, Höglinger, Trenkwalder, J Neurol Nov 2024): incorporates MDS clinical diagnostic criteria + α-synuclein seed amplification assay as ancillary biomarker; sets new diagnostic threshold framework.
- International cognitive disorders in PD best-practice guidelines (Goldman et al, Age Ageing 2026): standardises diagnosis and management of mild cognitive impairment in PD and PD-dementia; rivastigmine remains first-line cholinesterase inhibitor; pimavanserin preferred over quetiapine for psychosis in cognitively impaired patients. [PMID 41870152]
- Spanish expert consensus on DA agonist therapy in PD (Mir et al, Neurologia 2023): practical algorithm for choosing among pramipexole, ropinirole, rotigotine, and apomorphine across early, advanced, and special-population scenarios; emphasises rotigotine patch where swallowing is problematic and apomorphine pump in fluctuating advanced disease. [PMID 37419211]
- MDS-UPDRS Part III meaningful motor progression threshold (Holden et al, J Parkinsons Dis 2025): clinically meaningful threshold estimated at ~3.25 points OFF-medication; standardises trial endpoint interpretation. [PMID 39973477]
RA 6. Indian Regulatory & Society Actions
- Foslevodopa-foscarbidopa (Vyalev / Produodopa) — not yet CDSCO-approved in India; AbbVie has stated regulatory submission is in progress for the Indian market (manufacturer communication 2024). The 2024 Indian movement-disorders community has tracked the EU/US approval closely. [AbbVie 2024]
- Apomorphine pump (Apokyn / Apomine) — continues as the only continuous-infusion device-aided therapy widely available in India since the Nanavati launch 2019–20; remains the operational alternative to overseas LCIG/Vyalev for advanced-PD patients in Indian practice.
- Pimavanserin appears in the CDSCO 2024 new-drug approvals list under "Parkinson's disease psychosis" indication; no Indian-manufactured branded form widely available yet — currently imported as Nuplazid. [CDSCO 2024]
- Annals of Indian Academy of Neurology 2023 Supplement (Suppl 1, Vol 26) dedicated issue on PD: multi-modal rehabilitation review, deep brain stimulation outcomes from Indian centres, atypical parkinsonism series — useful Indian-context reference material for thesis citation work.
- ICMR-NCDIR PD epidemiology data (latest 2024 release) estimates Indian PD prevalence at ~70–100 per 100,000, with a younger mean age at onset (~58 years) than Western cohorts — a recurring point in Indian theses. [ICMR 2024]
Multi-source disagreements
- Levodopa BBB transit fraction without DDC inhibitor: KDT 8e gives 1–2 %; Katzung 16e and G&G 14e give 1–3 %. Minor — both indicate that the vast majority is decarboxylated peripherally. Treat as approximate.
- Trihexyphenidyl daily dose: KDT 8e gives 2–10 mg; Katzung 16e gives 6–20 mg. Indian clinical practice generally follows the lower KDT range; both ranges are acceptable for exam purposes.
- Selegiline neuroprotection: KDT presents the DATATOP-era hypothesis as still under evaluation; Katzung notes that subsequent large trials have failed to detect a difference in disease progression. Modern position is that selegiline is symptomatic-only; the rasagiline ADAGIO 1 mg arm produced equivocal but more promising data.
- Carbidopa "ceiling" dose for nausea suppression: KDT cites ~75 mg/day; Katzung notes that supplemental carbidopa (Lodosyn 25 mg) can be added beyond the standard combination's contribution if nausea persists.
- Pramipexole vs ropinirole potency: KDT calls pramipexole twice as potent as ropinirole; Katzung describes them as comparable in efficacy. Use the consensus framing: "comparable efficacy and tolerability; pramipexole is twice as potent on a milligram basis."