Antiparkinsonian Drugs
Pharmacotherapy of Parkinson's disease — levodopa, dopaminergic agents, anticholinergics, recent advances
Past RGUHS + DNB + MPMSU + MUHS · 31
RGUHSMar '26
MPMSUJan '25
DNBApr '23
DNBOct '23
MUHSWinter '22
DNBDec '21
MUHSSummer '21
RGUHSNov '20
RGUHSJun '20
MPMSU2019
MPMSUMay '19
MUHSWinter '19
RGUHSNov '17
MPMSU2017
MUHSSummer '17 Suppl
RGUHSNov '16
MUHSSummer '16
DNBDec '14
RGUHSOct '10
MPMSU2010
MPMSU2010
RGUHSOct '09
RGUHSMay '09
RGUHSApr '08
RGUHSApr '07
MPMSU2006
MPMSU2005
MPMSU2005
MPMSU1998
MPMSU1995
MPMSU1992
Introduction
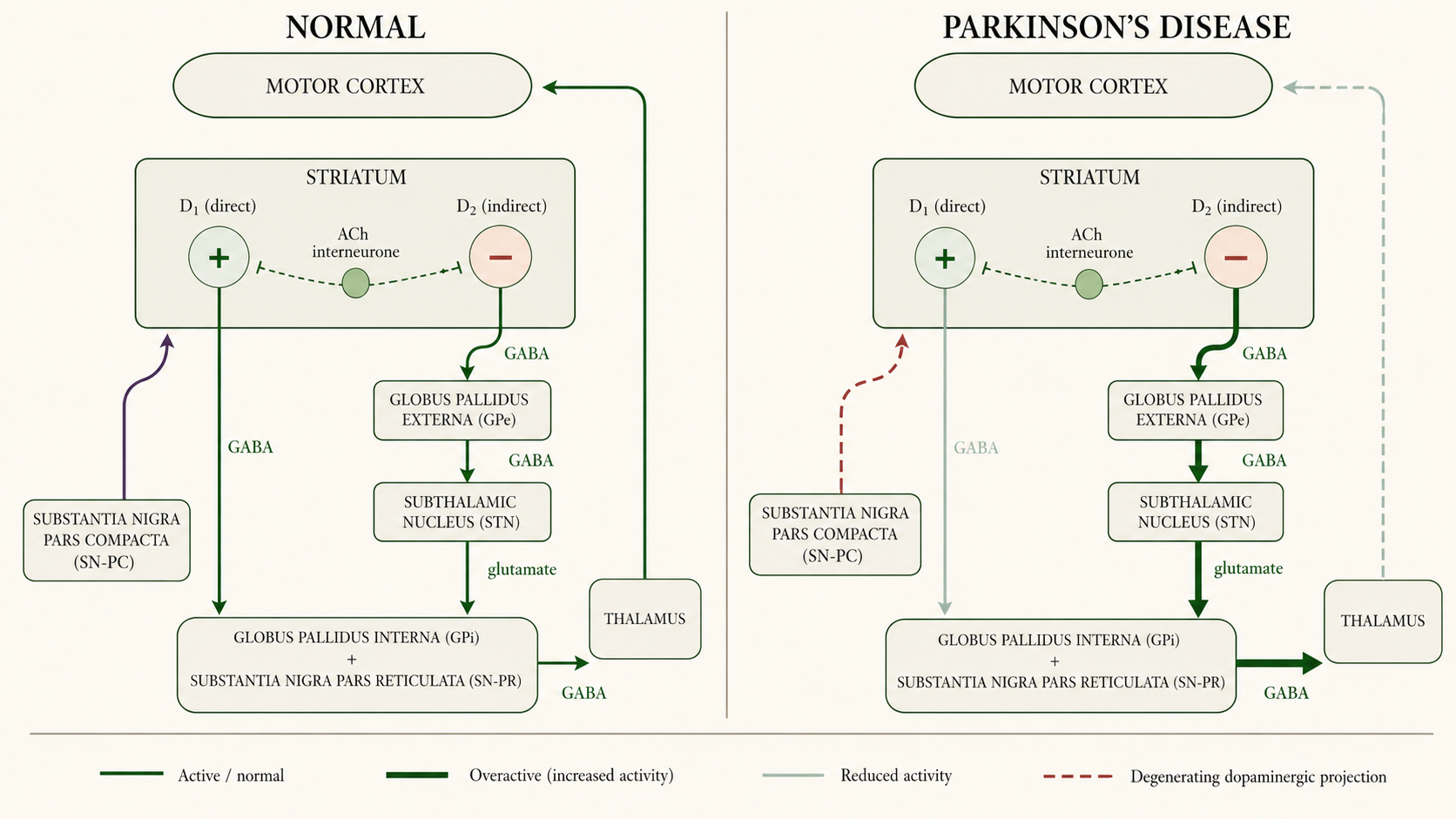
- Parkinson's disease — extrapyramidal disorder defined by the tetrad of rigidity, tremor, hypokinesia/bradykinesia, and postural instability; secondary mask facies, sialorrhoea, defective gait.
- Pathological hallmark — loss of pigmented dopaminergic neurones of the substantia nigra pars compacta (SN-PC) with intracellular Lewy bodies whose principal aggregate is α-synuclein — PD is a synucleinopathy.
- Symptom threshold — 70–80 % loss of SN-PC dopaminergic neurones; the resulting striatal DA depletion unbalances the dopaminergic-cholinergic equilibrium driving bradykinesia.
- Therapeutic principle — restore striatal DA tone or suppress unbalanced cholinergic activity. No available drug alters the underlying pathology — disease continues to progress.
- Pharmacotherapy impact — drugs add 5–10 years of better-quality life and lower mortality when initiated early.
Classification
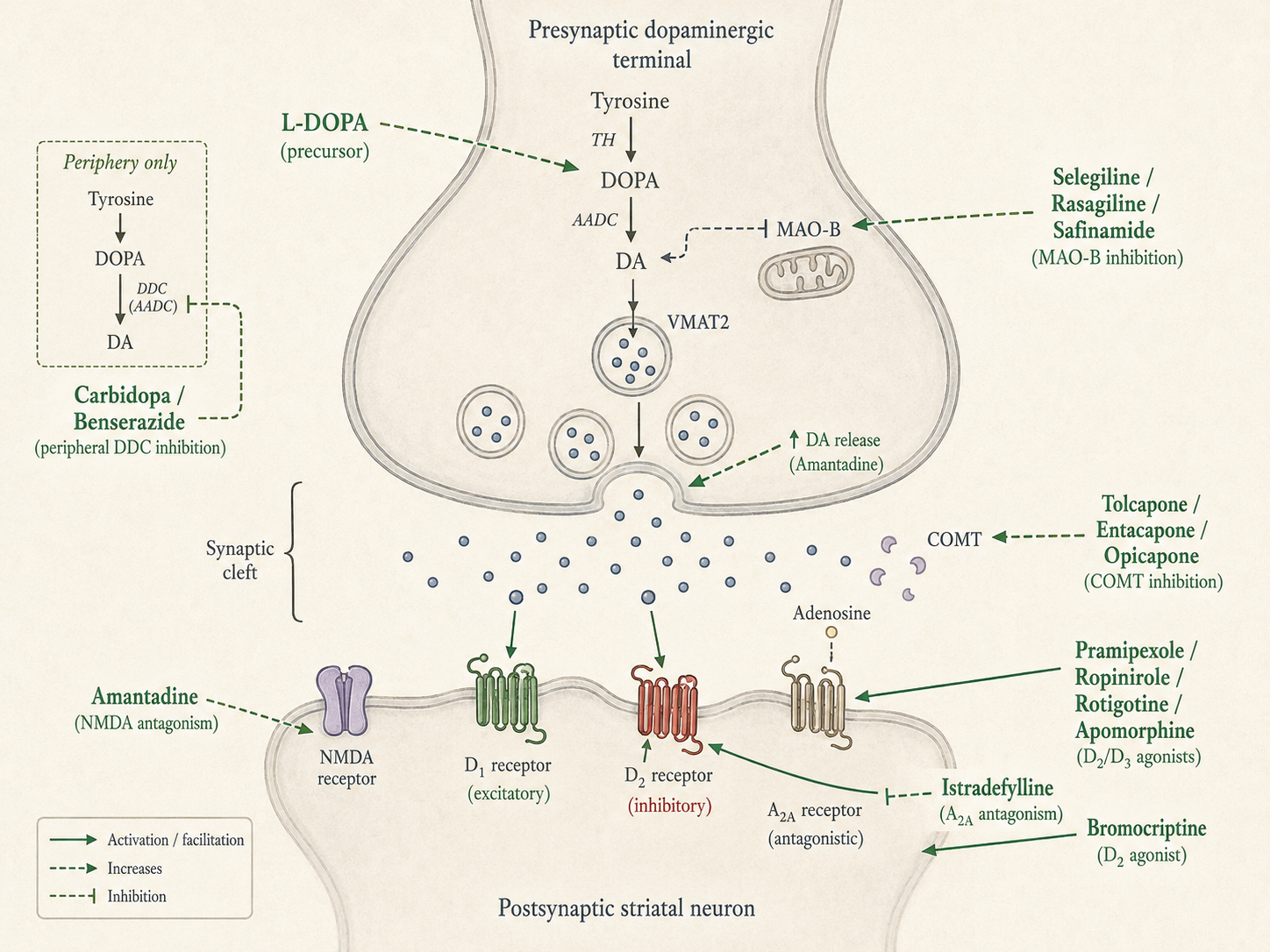
- DA precursor — Levodopa (the immediate metabolic precursor of dopamine; crosses the BBB whereas DA itself does not).
- Peripheral DDC inhibitors — Carbidopa, Benserazide — adjuvants that do not cross the BBB; reduce required levodopa by ~75 %.
- DA agonists — ergot — Bromocriptine, Pergolide (pergolide withdrawn in US — valvulopathy).
- DA agonists — non-ergot — Pramipexole, Ropinirole (oral); Rotigotine (transdermal); Apomorphine (SC rescue).
- MAO-B inhibitors — Selegiline, Rasagiline, Safinamide.
- COMT inhibitors — Entacapone, Tolcapone, Opicapone.
- NMDA antagonist / DA facilitator — Amantadine — multi-modal.
- Adenosine A2A antagonist — Istradefylline — caffeine analogue, adjunct for off-periods.
- Central anticholinergics — Trihexyphenidyl (benzhexol), Procyclidine, Biperiden, Benztropine; antihistaminics with central anticholinergic action — Promethazine, Orphenadrine, Diphenhydramine.
Levodopa & Carbidopa
- Most efficacious single agent — in PD — efficacy exceeds any other antiparkinsonian drug used alone; 1967 Cotzias breakthrough.
- Why not give DA — DA does not cross the BBB; levodopa crosses via the L-aromatic amino acid transporter (LAT).
- Fate without DDC inhibitor — >95 % decarboxylated peripherally; only 1–3 % reaches the brain — the basis for combining with a peripheral DDC inhibitor.
- Central conversion — levodopa → DA via AADC in surviving nigrostriatal terminals; stored in vesicles via VMAT2; released as transmitter. Surviving terminals provide the buffering capacity whose loss drives motor fluctuations.
- Pharmacokinetics — rapid small-bowel absorption via the LAA carrier — competes with dietary protein for absorption and BBB transport; Tmax 0.5–2 h; t½ 1–3 h; ~⅔ excreted as urinary HVA/DOPAC within 8 h.
- Slow gastric emptying or high gastric pH ↓ bioavailability.
- 3-OMD (COMT-derived) competes with levodopa for active BBB transport.
- Carbidopa / benserazide — extracerebral DDC inhibitors that do not cross the BBB — prolong levodopa t½, reduce dose by ~75 %, smoother CNS levels, ↓ on-off, abolish pyridoxine reversal, ↓ peripheral DA-mediated nausea/arrhythmia. Carbidopa ~75 mg/day saturates peripheral DDC; supplemental Lodosyn 25 mg if nausea persists.
- Standard dosing — Co-careldopa (LD 100 mg + CD 25 mg) TDS, titrated to LD 0.4–0.8 g/day; initiate 30–60 min before meals. Indian brands SYNDOPA, TIDOMET, SINEMET; benserazide combination MADOPAR.
- Newer formulations — Sinemet CR (sustained release); Rytary (extended-release CD/LD beads); Stalevo (LD + CD + entacapone); Duodopa intestinal gel (PEG-J pump for advanced PD); Inbrija (inhaled levodopa for off-rescue).
- AEs at initiation — nausea/vomiting in ~80 % on monotherapy (falls to <20 % with carbidopa via reduced peripheral DA at the CTZ); postural hypotension in ~⅓; arrhythmias and angina in IHD; tolerance to most early effects.
- Motor complications (chronic) — dyskinesias in up to 80 % by 10 years (choreoathetoid; pulsatile-stimulation hypothesis — lower incidence with continuous delivery); wearing-off (end-of-dose); on-off phenomenon (rapid unpredictable switches reflecting loss of buffering capacity).
- Behavioural / psychiatric — anxiety, vivid dreams, hallucinations, mania, confusion, psychosis from excess limbic DA; pimavanserin 34 mg/day (selective 5-HT2A inverse agonist) or atypical antipsychotics with low D2 affinity (clozapine, quetiapine) preferred; conventional D2 blockers contraindicated; black-box mortality risk in dementia-related psychosis.
- Contraindications — angle-closure glaucoma, active psychosis, melanoma history; cautious in IHD, cerebrovascular disease, peptic ulcer, gout; do not stop abruptly — risk of NMS-like syndrome.
- Interactions — Pyridoxine abolishes monotherapy effect (peripheral DDC enhancement) — eliminated by carbidopa; non-selective MAOIs → hypertensive crisis (stop ≥14 d before); D2-blocker antiemetics (metoclopramide, phenothiazines) reverse benefit — use domperidone instead (acts at CTZ outside BBB without CNS effect); reserpine abolishes action (VMAT2 block); antihypertensives potentiate postural hypotension.
DA agonists, MAO-B, COMT, amantadine, A2A antagonist
- DA agonists — rationale — act directly on postsynaptic striatal DA receptors — independent of surviving terminals; longer-acting than levodopa; subtype-selective; no oxidative metabolism; no amino-acid competition.
- vs Levodopa — less symptomatic benefit but lower dyskinesia rate as initial monotherapy (PD MED 2014); higher rate of mental AEs, somnolence, peripheral oedema, and impulse-control disorders. Disappointing if patient never responded to levodopa.
- Pramipexole — non-ergoline; D2/D3 selective with greater D3 affinity; 0.5–1.5 mg TDS; renal excretion → renal dose-adjust; possible mood-elevating effect.
- Ropinirole — non-ergoline; D2-selective; CYP1A2 metabolism (ciprofloxacin ↑ levels; smoking ↓); 2–8 mg TDS; FDA-approved for restless legs syndrome.
- Rotigotine, Apomorphine — rotigotine — 24-h transdermal D2/D1 patch giving continuous stimulation. Apomorphine — SC rescue for off-periods, onset ~10 min; antiemetic premedication (trimethobenzamide) needed; contraindicated with 5-HT3 antagonists (ondansetron) — risk of profound hypotension/syncope.
- ICDs — compulsive gambling, shopping, sexual behaviour, eating; up to 45 % on DA agonists via D2/D3 mesocorticolimbic activation; risk factors male sex, younger age, prior addictive behaviour; actively screen — under-reported; resolve on withdrawal.
- DAWS — DA-agonist withdrawal syndrome — anxiety, panic, depression, autonomic features, drug cravings; refractory to levodopa, may persist months; never stop a DA agonist abruptly. Sleep attacks documented with pramipexole/ropinirole — driving caution. [PMID 37147135]
- MAO-B — selegiline — irreversible MAO-B inhibitor at ≤10 mg/day → ↓ intracerebral DA degradation; no cheese reaction at therapeutic dose; metabolised to L-amphetamine/methamphetamine → insomnia (give morning + lunch only); pethidine → excitement, hyperthermia; avoid TCAs/SSRIs/tramadol.
- Rasagiline, Safinamide — Rasagiline — 5× more potent than selegiline, OD, no amphetamine metabolites — preferred; ADAGIO 1 mg arm suggested possible disease modification (equivocal). Safinamide — reversible MAO-B + glutamate-release inhibition; adjunct only for wearing-off.
- COMT inhibitors — adjuncts in motor fluctuations — prolong levodopa t½, ↑ ON-time, ↓ OFF-time; do not change peak/Tmax; lower LD dose 20–30 % to prevent dyskinesia/nausea; not for early therapy.
- Specific COMT agents — Entacapone — peripheral-only, with each LD dose; preferred. Tolcapone — central+peripheral, more potent but black-box hepatotoxicity (LFT q2–4 wk); restricted to entacapone non-responders. Opicapone — long-acting OD bedtime via slow dissociation despite short t½.
- Amantadine — multi-modal: enhances presynaptic DA release, NMDA antagonism (key niche — suppresses LD-induced dyskinesia), anticholinergic, and adenosine A2A antagonism. 100 mg BD; livedo reticularis + ankle oedema characteristic; caution in seizure history, heart failure, renal impairment.
- Istradefylline — selective adenosine A2A receptor antagonist; A2A and D2 form heterodimers in striatum — A2A block boosts dopaminergic tone. 20 or 40 mg PO OD; adjunct for off-periods, not effective as monotherapy.
Central Anticholinergics
- Class profile — trihexyphenidyl, procyclidine, biperiden, benztropine — central > peripheral muscarinic antagonism; ↓ unbalanced cholinergic-interneurone activity in striatum, restoring DA/ACh balance.
- Symptom profile — tremor benefits more than rigidity; hypokinesia improves least; sialorrhoea controlled by peripheral antimuscarinic action; 10–25 % overall improvement after a single dose.
- Drugs of choice — for drug-induced (D2-antagonist) parkinsonism — only effective class in this setting; levodopa is unhelpful while neuroleptics continue and may aggravate underlying psychiatric illness.
- Adverse effects — poorly tolerated in elderly — memory/cognition impairment, organic confusional states, blurred vision, urinary retention (especially elderly males), constipation, suppurative parotitis from xerostomia.
- Withdraw gradually — abrupt cessation may exacerbate parkinsonism. Antihistaminics (orphenadrine, diphenhydramine, promethazine) — milder, better tolerated in older patients; sedative effect helps in some.
Treatment Approach & Motor-fluctuation Management
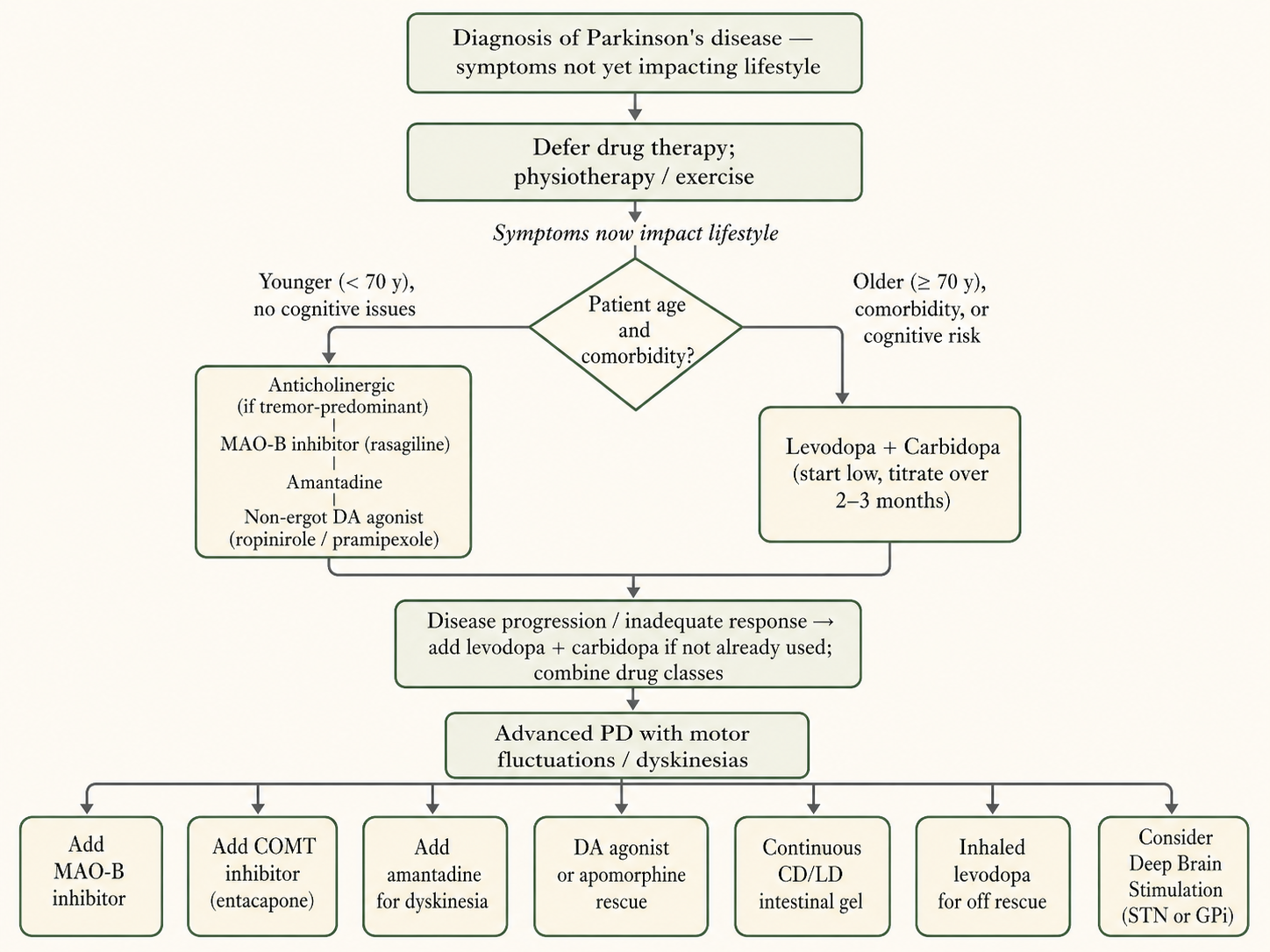
- Step 1 — pre-pharmacologic — exercise, physiotherapy, education; many authorities now recommend delaying dopaminergic initiation until symptoms impact lifestyle.
- Step 2 — mild PD — anticholinergics (younger, tremor-predominant), MAO-B inhibitor (selegiline/rasagiline), amantadine, or non-ergot DA agonist.
- Step 3 — younger patients — non-ergot DA agonist (pramipexole/ropinirole) monotherapy to delay levodopa exposure and motor complications.
- Step 4 — older (>70 y) or comorbid — start LD/CD directly — better tolerated; AAN 2021 (reaffirmed Feb 2025) endorses levodopa-first for motor symptom control in early PD. [AAN 2021/2025]
- Wearing-off management — dose fractionation; add MAO-B (rasagiline preferred); add COMT (entacapone with each LD dose); add DA agonist; switch to ER LD/CD (Rytary); evening protein redistribution to ↓ daytime fluctuations.
- Off-period rescue — apomorphine SC (test dose required; antiemetic premed); inhaled levodopa (Inbrija); for refractory advanced PD — Duodopa LCIG (intrajejunal CD/LD) or foslevodopa-foscarbidopa SC pump (Vyalev — see RA).
- Dyskinesias — amantadine first-line antidyskinetic; clozapine second-line; continuous delivery (rotigotine patch, intrajejunal LD); drug holidays no longer practiced.
- Surgical & non-motor — DBS (STN > GPi) for moderate PD with refractory motor fluctuations; MRgFUS thalamotomy for medication-refractory tremor; rivastigmine/donepezil/memantine for cognition; SSRIs for affective symptoms; pimavanserin for psychosis. Abrupt LD or DA-agonist withdrawal can precipitate NMS-like syndrome.
Recent Advances
- Foslevodopa–foscarbidopa (Vyalev / Produodopa) — AbbVie; FDA approval 17 Oct 2024 — first subcutaneous 24-h continuous infusion levodopa therapy via the Vyafuser pump for advanced-PD motor fluctuations; non-surgical alternative to LCIG. Pivotal phase-3 (Soileau et al, Lancet Neurol 2022): +1.79 h ON-time without troublesome dyskinesia, −1.79 h OFF-time vs oral IR LD/CD; skin reactions are the principal tolerability issue. [FDA 2024-Oct] [PMID 36402160]
- Tavapadon (TEMPO programme) — selective D1/D5 partial agonist — mechanistically distinct from D2/D3 agonists, theoretically avoiding ICDs and somnolence. TEMPO-3 (2024) phase-3 adjunctive met primary endpoint: +1.1 h additional ON-time without troublesome dyskinesia vs placebo (1.7 vs 0.6 h; p < 0.0001); TEMPO-1/-2 confirmed monotherapy efficacy in early PD; NDA filed 2026. [AbbVie 2024]
- LIXIPARK — GLP-1 RA disease modification — Meissner, Rascol et al, NEJM 2024 phase-2: 156 early-PD patients; lixisenatide 20 µg SC daily for 12 months; MDS-UPDRS Part III change +0.04 vs +3.04 placebo (between-group 3.08, 95 % CI 0.86–5.30; p = 0.007). First positive disease-modifying GLP-1 signal; offset by nausea 46 %, vomiting 13 %. [PMID 38598572]
- Exenatide-PD3 — negative phase 3 — Vijiaratnam, Foltynie et al, Lancet 2025: exenatide 2 mg SC weekly × 96 weeks in 194 moderate-PD patients — no significant difference in MDS-UPDRS Part III off-medication progression. Tempers GLP-1 enthusiasm; class effect in PD remains unproven. [Lancet 2025]
- Prasinezumab (PASADENA + PADOVA) — humanised anti-aggregated-α-synuclein mAb; both trials missed formal primary endpoints but showed supportive trends (40–64 % motor-decline reduction in MAO-B subgroup); Roche advanced to phase 3 on 16 Jun 2025 (n = 900, completion 2029). Cinpanemab — another anti-synuclein mAb — phase-2 negative; not all anti-synuclein antibodies behave alike. [Roche 2025-Jun] [PMID 35921450]
- FAIRPARK-II — deferiprone NEGATIVE/HARMFUL — Devos et al, NEJM 2022: iron chelator deferiprone 30 mg/kg/day in 372 newly-diagnosed PD worsened motor function (+2.6 MDS-UPDRS Part III points at 36 weeks). Closes iron-chelation as a near-term disease-modifying strategy. [PMID 36449420]
- AAN Practice Guideline 2021 (reaffirmed Feb 2025) — levodopa is the preferred initial dopaminergic therapy for motor symptom control in early PD; DA agonists carry higher risk of ICDs, somnolence, oedema, hallucinations; MAO-B inhibitors are an option for very mild symptoms. ICD risk factors: male sex, younger age, prior ICDs, mood disorder, family history of gambling/addiction. [AAN 2021/2025]
- Indian context — Vyalev not yet CDSCO-approved (regulatory submission in progress, AbbVie 2024); apomorphine pump (Apokyn/Apomine) remains the only continuous-infusion device-aided therapy widely available in India since the Nanavati 2019–20 launch; pimavanserin appears in CDSCO 2024 new-drug approvals for PD psychosis (currently imported as Nuplazid). ICMR-NCDIR 2024 estimates Indian PD prevalence ~70–100 per 100,000 with younger mean age at onset (~58 y) than Western cohorts. [CDSCO 2024] [ICMR 2024]
![Figure 4 [RA] — Three modes of continuous-delivery levodopa: oral immediate-release (pulsatile) vs intrajejunal LCIG (Duodopa, PEG-J) vs subcutaneous foslevodopa–foscarbidopa pump (Vyalev / Produodopa, Vyafuser pump).](images/antiparkinsonian-drugs/pharma_parkinsons-disease_ra_01_foslevodopa-foscarbidopa-subcutaneous-pump.png)
Mnemonic — Six pharmacological strategies in PD
- 1. Replace DA — Levodopa (+ carbidopa/benserazide).
- 2. Mimic DA — DA agonists — pramipexole, ropinirole, rotigotine, apomorphine; ergot bromocriptine.
- 3. Spare endogenous DA — MAO-B (selegiline, rasagiline, safinamide) + COMT (entacapone, tolcapone, opicapone).
- 4. Modulate the circuit — Amantadine (NMDA antagonist — also key antidyskinetic) + Istradefylline (A2A antagonist).
- 5. Restore ACh balance — Central anticholinergics (trihexyphenidyl, benztropine) — drugs of choice for drug-induced parkinsonism.
- 6. Surgical / device-aided — DBS (STN/GPi); MRgFUS thalamotomy; LCIG (Duodopa); SC pump (Vyalev).
Clinical pearls
- Domperidone exploits the BBB — controls levodopa-induced nausea without abolishing the antiparkinsonian effect — acts at the CTZ which sits outside the BBB.
- Pyridoxine paradox — B6 abolishes levodopa monotherapy via peripheral DDC enhancement, but the effect is eliminated when carbidopa is co-administered.
- Carbidopa ceiling — ~75 mg/day saturates peripheral DDC; supplemental Lodosyn 25 mg can be added when nausea persists despite a standard combination dose.
- Never stop a DA agonist abruptly — DAWS (DA-agonist withdrawal syndrome) is refractory to levodopa and may persist months — taper slowly.
- Drug-induced parkinsonism — stop the offender if possible; anticholinergics are the only effective class — levodopa is ineffective while neuroleptics continue and may aggravate underlying psychotic illness.
Table 1 — Initial therapy options compared (basis for AAN 2021/2025, PD MED 2014)
| Option | Symptomatic benefit | Dyskinesias / motor complications | Mental AEs / ICDs | Best for |
|---|---|---|---|---|
| Levodopa + carbidopa/benserazide | Highest of all classes | Highest dyskinesia rate over time (up to 80 % by 10 y) | Lower psychiatric burden than DA agonists | Older (>70 y) or all-comers per AAN 2021/2025 |
| Non-ergot DA agonist (pramipexole, ropinirole, rotigotine) | Less than levodopa | Lower dyskinesia rate as initial monotherapy | Highest ICDs, somnolence, peripheral oedema | Younger PD; levodopa-sparing strategy |
| MAO-B inhibitor (rasagiline, selegiline) | Mildest of the three | Minimal motor complications | Insomnia (selegiline amphetamine metabolites) | Very mild early PD; possible neuroprotection (rasagiline ADAGIO equivocal) |
References & further reading
- KD Tripathi — Essentials of Medical Pharmacology, 8e (2018), Ch.31 — Drugs for Parkinsonism.
- Goodman & Gilman — The Pharmacological Basis of Therapeutics, 14e (2023), Ch.21 — Treatment of CNS Degenerative Disorders.
- Katzung — Basic & Clinical Pharmacology, 16e (2023), Ch.28 — Pharmacologic Management of Parkinsonism & Other Movement Disorders.
- Pringsheim et al. — AAN Practice Guideline: Dopaminergic therapy for motor symptoms in early PD. Neurology 2021; reaffirmed 8 Feb 2025.
- Soileau et al. — Foslevodopa–foscarbidopa pivotal phase-3 trial. Lancet Neurol 2022. [PMID 36402160]
- Meissner, Rascol et al. — LIXIPARK phase-2 lixisenatide trial. NEJM 2024. [PMID 38598572]