Classification of Antihistamines
H₁–H₄ antagonists · generations · chemical classes · newer agents and their advantages
Past RGUHS · 2
RGUHS2023
RGUHS2017
Introduction
- Definition — Antihistamines are drugs that antagonise histamine at its receptors; the unqualified term means the H1 antihistamine, the mainstay of urticaria and histamine-mediated pruritus.
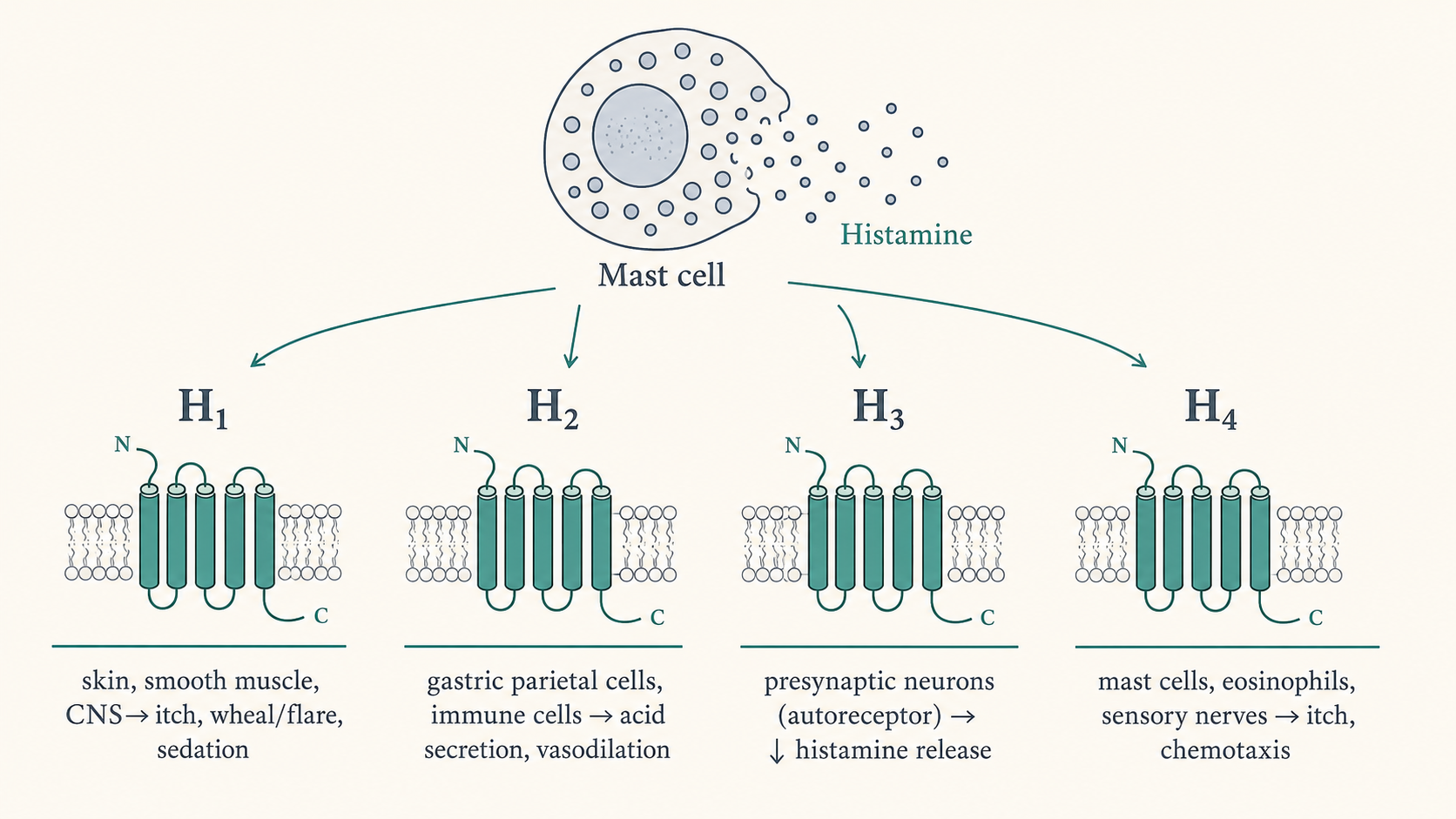
- Histamine acts through four GPCR subtypes — H1, H2, H3, H4 — so the antihistamine family spans four pharmacological targets, of which H1 and H2 are in routine dermatologic use.
- More than 45 H1 antihistamines exist worldwide; in DVL they treat urticaria, angioedema, pruritus, drug/food allergy, mastocytosis and allergic rhinitis/conjunctivitis.
Classification
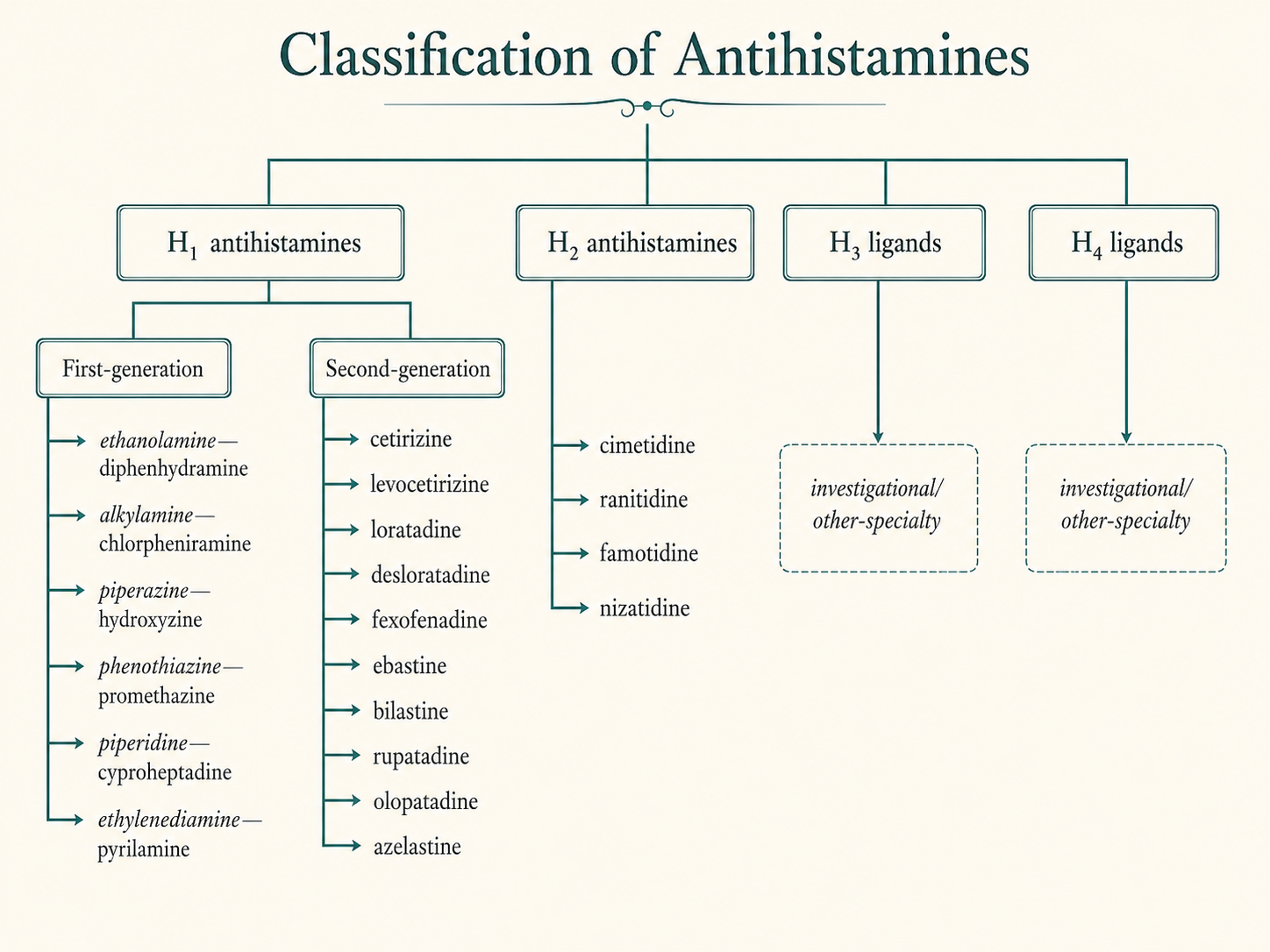
- Axis A — by receptor target — H1 antagonists (conventional antihistamines) · H2 antagonists (cimetidine, ranitidine, famotidine, nizatidine) · H3 ligands (autoreceptor; CNS) · H4 ligands (investigational antipruritic).
- Axis B — H1 agents by generation — First-generation (sedating, non-selective, short-acting) vs second-generation (non-sedating, H1-selective, long-acting); a so-called third-generation (active metabolites/enantiomers) is not accepted as a distinct class.
- Axis C — by chemical structure — Ethanolamines (diphenhydramine) · ethylenediamines (pyrilamine) · alkylamines (chlorpheniramine) · piperazines (hydroxyzine, cetirizine) · piperidines (cyproheptadine, loratadine, fexofenadine) · phenothiazines (promethazine) · phthalazinones (azelastine).
Histamine receptors and their antihistamine relevance (basis of the receptor-target classification)
| Receptor | G-protein / messenger | Key effects | Antagonist examples |
|---|---|---|---|
| H1 | Gq → IP3/DAG, ↑Ca2+ | Itch, wheal/flare, vasodilation, bronchoconstriction, CNS arousal | Cetirizine, fexofenadine, chlorpheniramine |
| H2 | Gs → ↑cAMP | Gastric acid; minor cutaneous vasodilation | Cimetidine, ranitidine, famotidine |
| H3 | Gi → ↓cAMP | Presynaptic autoreceptor — ↓ histamine release | Thioperamide, pitolisant (CNS) |
| H4 | Gi → ↓cAMP | Mast-cell/eosinophil chemotaxis, itch | JNJ-39758979, toreforant, adriforant (investigational) |
Mechanism of action
- Inverse agonism — H1 (and H2) antihistamines are inverse agonists — they bind and stabilise the inactive receptor conformation, down-regulating its constitutive activity (not simple competitive blockade).
- Anti-inflammatory effect — Via the H1 receptor they also ↓ pro-inflammatory cytokines (TNF-α, IL-6, IL-8), ↓ adhesion molecules (ICAM-1, VCAM-1) and ↓ eosinophil chemotaxis — most evident at higher doses.
- Palliative only — They block the effects of released histamine but do not prevent histamine release or the antigen–antibody reaction.
First-generation H1 antihistamines
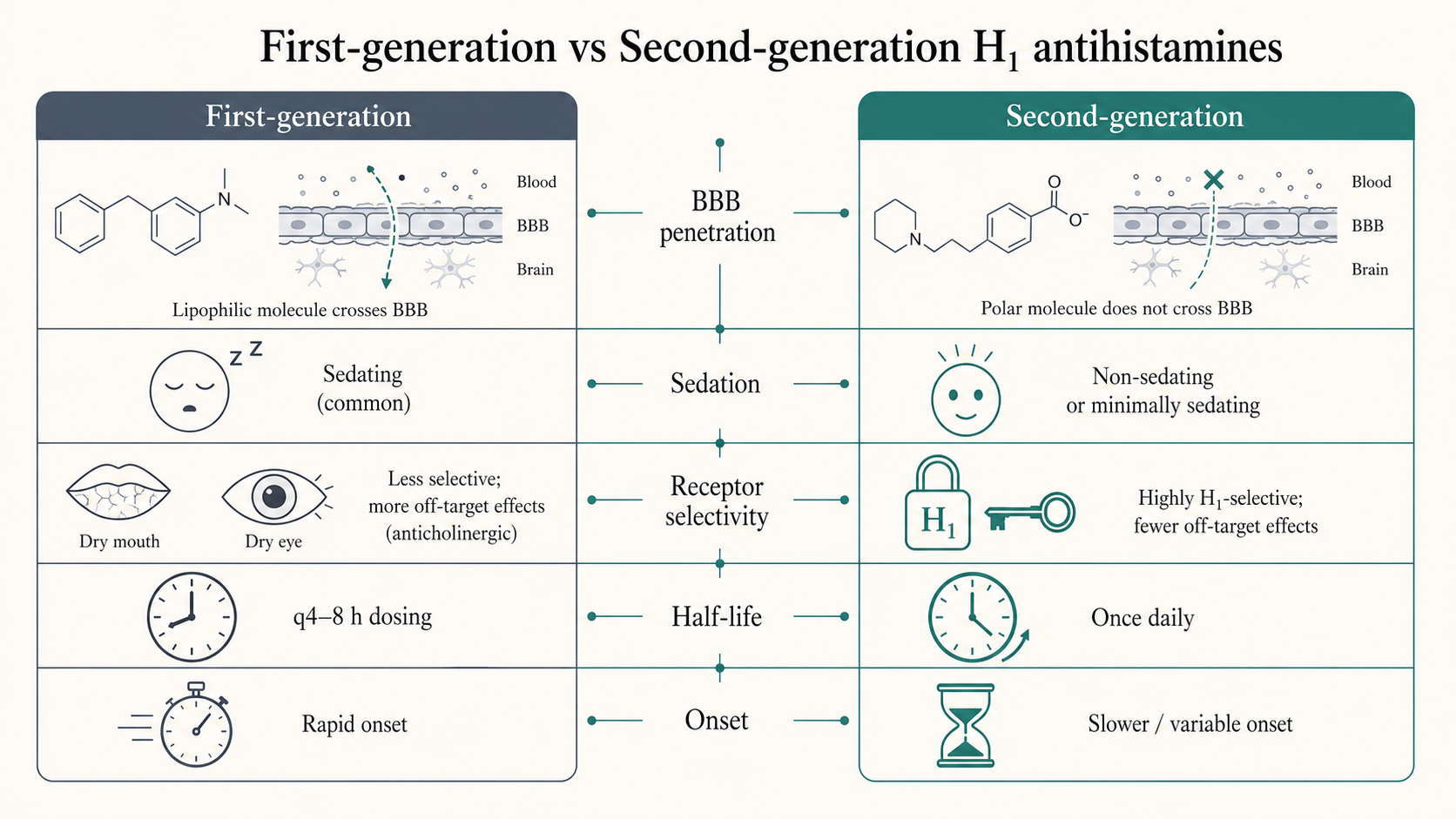
- Defining features — Lipophilic → cross the blood–brain barrier (sedation); non-selective → anticholinergic, anti-α-adrenergic, anti-serotonergic, local-anaesthetic actions; short-acting (q4–8h).
- By chemical class (examples) — Ethanolamine — diphenhydramine, dimenhydrinate; piperidine — cyproheptadine (antiserotonin, appetite gain); phenothiazine — promethazine (antiemetic; avoid <2 y); alkylamine — chlorpheniramine (least sedating); piperazine — hydroxyzine (antipruritic, anxiolytic).
- Caveats — Reduce REM sleep and next-day performance, increase accidents; the GA2LEN position paper flags avoidable risk. Contraindicated in narrow-angle glaucoma, BPH, with MAO inhibitors.
Second-generation antihistamines and their advantages
- Definition — Post-1980 H1 blockers that are non-/low-sedating, H1-selective (minimal anticholinergic effect) and long-acting (once daily); some carry additional antiallergic actions (↓ leukotrienes, PAF, cytokines).
- Newer agents (examples) — Fexofenadine, loratadine, desloratadine, cetirizine, levocetirizine, and the newest — ebastine, bilastine, rupatadine, mizolastine, azelastine, olopatadine.
- Advantages over first-generation — No/low sedation and no psychomotor impairment (driving not contraindicated); no anticholinergic effects; once-daily dosing improves compliance; no potentiation of alcohol/benzodiazepines; cardiac-safe (current agents lack the QT risk that withdrew terfenadine/astemizole).
- Metabolite/enantiomer chains — Hydroxyzine → cetirizine → (R-enantiomer) levocetirizine; loratadine → desloratadine; terfenadine → fexofenadine (these are the basis of the contested third-generation label).
- Dual-mechanism newer agents — Rupatadine = H1 + PAF antagonist; olopatadine / azelastine / ketotifen = H1 antagonist + mast-cell stabiliser; bilastine = no CYP metabolism, no food/CYP interaction.
- Caveat — Cetirizine and levocetirizine (piperazines) retain mild sedation in ~10–15%; fexofenadine and loratadine/desloratadine are the least sedating.
Pharmacological actions and dermatological uses
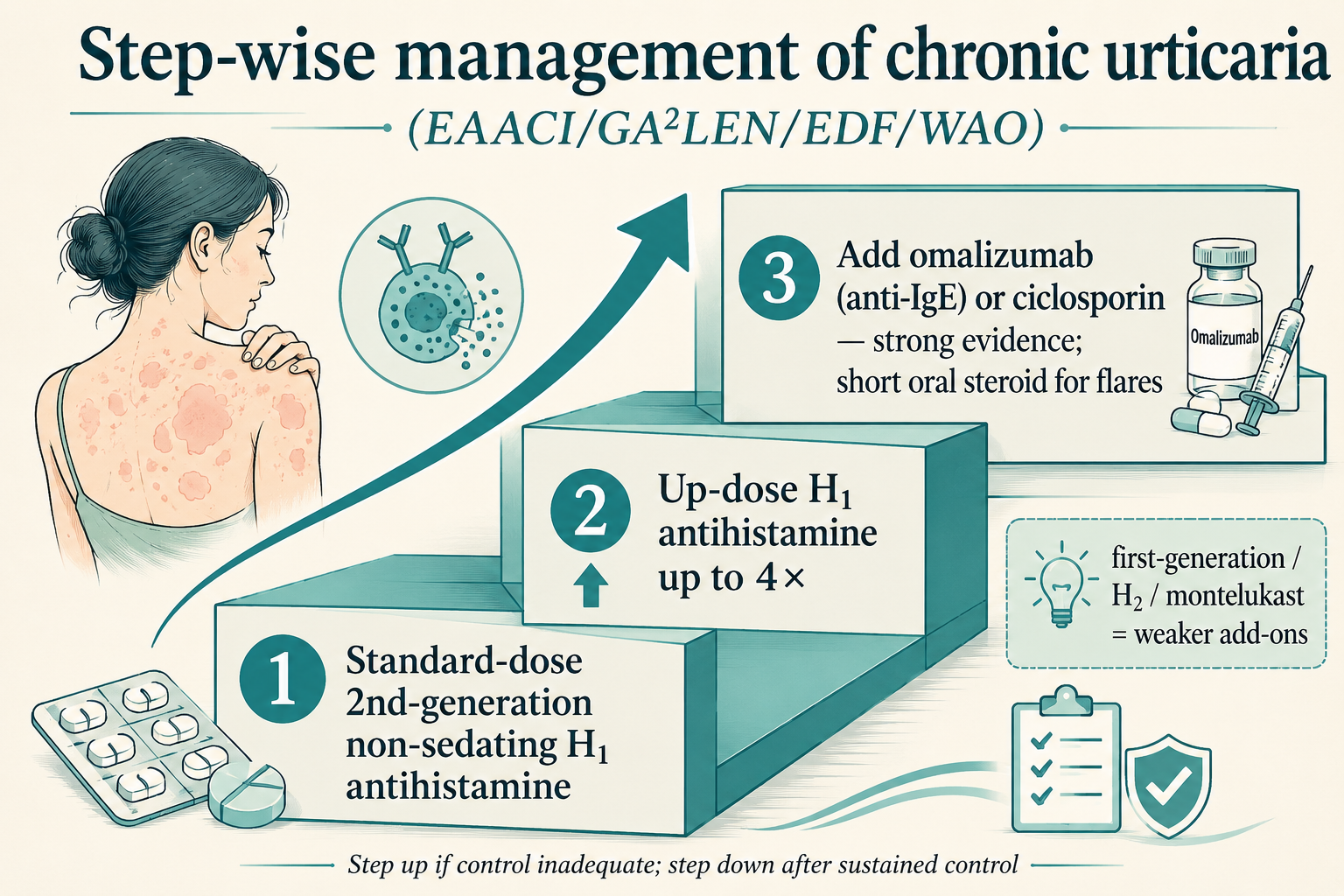
- Chronic spontaneous urticaria — Second-generation non-sedating H1 antihistamines are first-line; effective in ~50%. Stepwise ladder: standard dose → up-dose up to 4× → add omalizumab/ciclosporin.
- Pruritus — Useful where itch is histamine-mediated (urticaria, mastocytosis, insect bites); first-generation agents relieve nocturnal itch chiefly through sedation.
- Atopic dermatitis — Weak/ambiguous evidence — benefit is mainly the soporific effect; AAD discourages routine use; reserve for AD with concomitant urticaria/rhinitis.
- Other uses — Doxepin (TCA, dual H1/H2, 800× diphenhydramine) for refractory urticaria/pruritus; H2 antagonists as weak adjuncts; antihistamines as adjuncts (not primary) in anaphylaxis — adrenaline is first-line.
Adverse effects and precautions
- First-generation — Sedation, impaired cognition/psychomotor performance, paradoxical excitation in children; anticholinergic (dry mouth, urinary retention, blurred vision, constipation); postural hypotension; overdose mimics belladonna poisoning (excitation, convulsions).
- Second-generation — Generally well tolerated; mild sedation with cetirizine/levocetirizine; rare headache/GI upset.
- Cardiotoxicity (historical) — Terfenadine and astemizole withdrawn for QT prolongation/torsades (K+-channel block, worsened by CYP3A4 inhibitors); current agents are safe.
- Pregnancy/lactation — Chlorpheniramine and cetirizine/loratadine preferred (category B); avoid first-generation in lactation (sedation, ↓ milk).
Recent advances
- H4-receptor antagonists — JNJ-39758979 showed efficacy in atopic dermatitis/pruritus but was terminated for agranulocytosis; toreforant (no agranulocytosis) and adriforant (ZPL-3893787) are the clinical-stage H4 antipruritics. PMID 28233185
- H4R itch mechanism — The H4 receptor with TRPV1 mediates cadaverine-induced itch — reinforcing H4R as an antipruritic target distinct from H1. PMID 39079948
- H3 ligand pitolisant — The only marketed H3 inverse agonist — approved for narcolepsy, no dermatologic indication; betahistine remains the H1-analogue for Ménière's. PMID 39186901
- Dupilumab for CSU — Anti-IL-4Rα biologic — first new targeted CSU therapy in over a decade (LIBERTY-CSU CUPID); FDA-approved April 2025 (≥12 y), extended to children 2–11 y April 2026. FDA 2025-Apr · PMID 41706458
- Remibrutinib (oral BTK inhibitor) — FDA first approval 30 Sep 2025 for antihistamine-refractory CSU — an oral step-up beyond antihistamine up-dosing. PMID 41559488
- Barzolvolimab (anti-KIT) — Mast-cell-depleting mAb gave 71% well-controlled and 57% complete response in antihistamine-refractory CSU (phase 1b). PMID 40415544
- Guideline — EAACI/GA2LEN/EuroGuiDerm/APAAACI 2022 — second-generation antihistamines first-line, up-dose 4×, then omalizumab; first-generation agents not recommended for routine CSU. Bilastine approved by DCGI/CDSCO in India. PMID 35092619 · DCGI
Mnemonic — receptor G-protein coupling
"1-Q, 2-S, 3/4-i": H1 = Gq (IP3/DAG/Ca2+) · H2 = Gs (↑cAMP) · H3 and H4 = Gi (↓cAMP). First-gen sedation classes (KDT): Highly — diphenhydramine, dimenhydrinate, promethazine, hydroxyzine.
Clinical pearls
- Second-generation non-sedating H1 antihistamine is the single best answer to "drug of choice for chronic urticaria"; up-dose to 4× before escalating.
- Cetirizine = metabolite of hydroxyzine; it concentrates in skin → superior in urticaria/AD but mildly sedating.
- Terfenadine and astemizole are the classic "withdrawn for torsades" antihistamines — a favourite viva point.
- "No third-generation antihistaminic" — international consensus; the metabolite/enantiomer agents stay second-generation.
First- vs second-generation H1 antihistamines (the high-yield comparison)
| Feature | First-generation | Second-generation |
|---|---|---|
| BBB penetration / sedation | High / sedating | Low / non-sedating |
| H1 selectivity | Low (anticholinergic, anti-α, anti-5HT) | High (selective) |
| Duration / dosing | Short, q4–8h | Long, once daily |
| Extra antiallergic action | None | ↓ LT, PAF, cytokines (some) |
| Prototype | Diphenhydramine, chlorpheniramine | Fexofenadine, cetirizine, bilastine |
References and further reading
- IADVL — Textbook of Dermatology, 5e — Ch.96 Antipruritic Agents; Ch.37 Diagnosis and Management of Urticaria.
- Fitzpatrick — Dermatology in General Medicine, 9e — Ch.189 Antihistamines.
- Wolverton — Comprehensive Dermatologic Drug Therapy, 4e — Ch.32 Antihistamines.
- Recent Advances updated on — 2026-06-20 — PubMed, US-FDA, CDSCO/DCGI, EAACI/GA2LEN 2022.