Classification of Antihistamines
H₁–H₄ antagonists · generations · chemical classes · newer agents and their advantages
Past RGUHS · 2
RGUHS2023
RGUHS2017
Classification of Antihistamines
1. Definition, scope & terminology
- Antihistamines are drugs that antagonise the actions of histamine at its receptors; in clinical practice the unqualified term means the H1-receptor antihistamine, the workhorse of urticaria and histamine-mediated pruritus (Fitzpatrick's 9e Ch.189, p.3451).
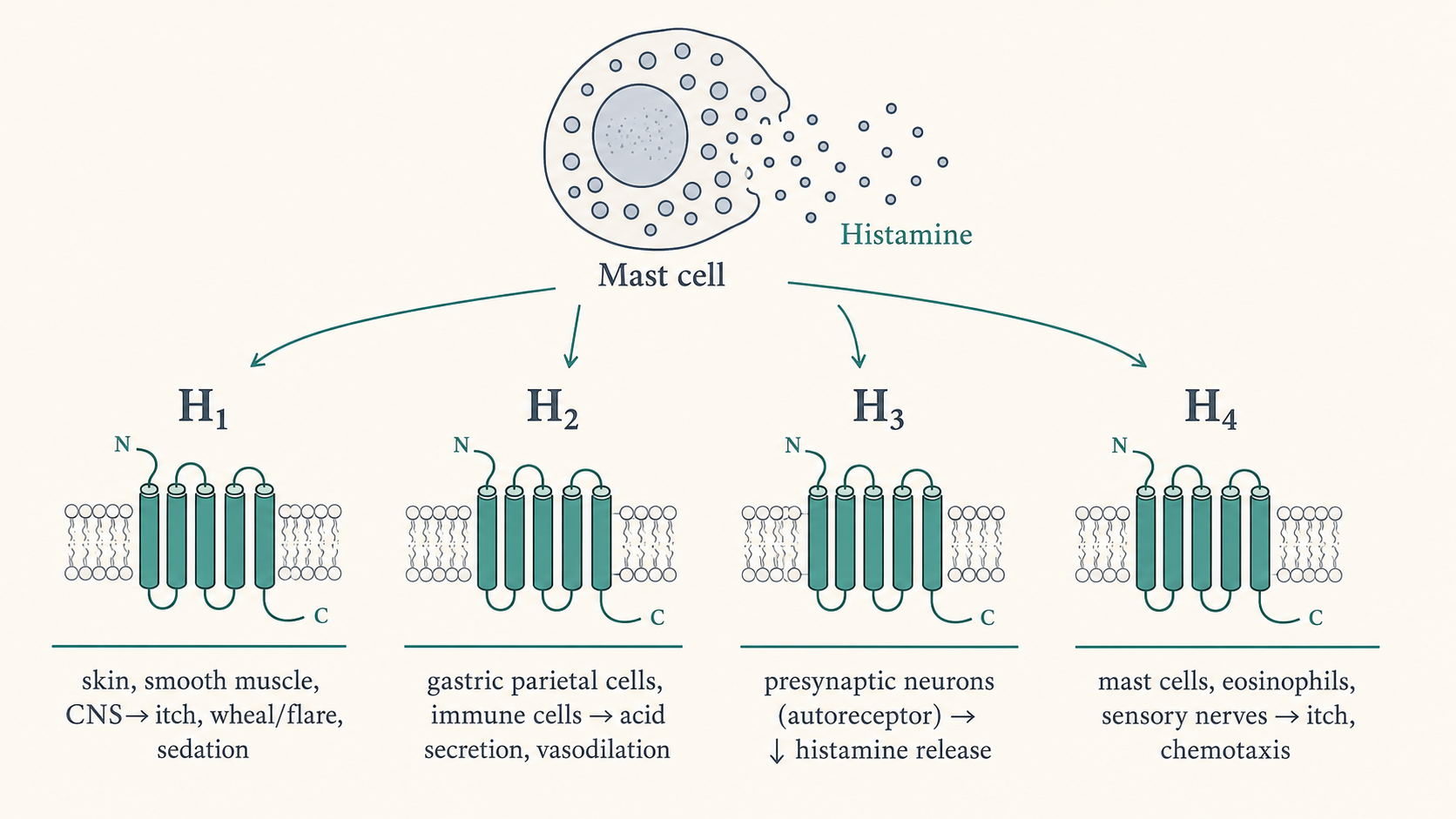
- Histamine acts through four G-protein–coupled receptor subtypes — H1, H2, H3, H4 — so "antihistamine" is properly a family spanning four pharmacological targets, only two of which (H1, H2) are in routine dermatologic use (Fitzpatrick's 9e Ch.189, p.3451; Wolverton 4e Ch.32, p.350).
- The principal axes of classification are: (i) by receptor target (H1 / H2 / H3 / H4 ligands); (ii) for H1 agents, by "generation" (first vs second, with a contested "third"); and (iii) by chemical class (ethanolamine, alkylamine, piperazine, piperidine, phenothiazine, ethylenediamine, phthalazinone) (Sardana Ch.3, Table 3.1; Fitzpatrick's 9e Ch.189, p.3451).
- More than 45 H1 antihistamines exist worldwide as prescription and over-the-counter agents — for urticaria, pruritus, allergic rhinitis/conjunctivitis, nausea, vertigo, sleep and anxiety (Fitzpatrick's 9e Ch.189, p.3451).
- A modern, mechanism-based reclassification has been proposed because old agents are inverse agonists (not simple "blockers") and because activity at non-H1 receptors (muscarinic, α-adrenergic, 5-HT, cardiac K+ channels) drives much of first-generation toxicity (Sardana Ch.3; Fitzpatrick's 9e Ch.189, p.3451).
2. Histamine and its receptors (the basis of classification)
- Histamine is a low-molecular-weight amine synthesised from L-histidine by histidine decarboxylase, stored noncovalently in mast-cell and basophil granules, and degraded by N-methylation (histamine-N-methyltransferase) or oxidative deamination (diamine oxidase) (Fitzpatrick's 9e Ch.189, p.3451; Wolverton 4e Ch.32, p.350).
- Histamine receptors are heptahelical (7-transmembrane) GPCRs with constitutive activity — they signal even without ligand; active and inactive states sit in equilibrium, shifted toward "active" by histamine and toward "inactive" by antihistamines (Fitzpatrick's 9e Ch.189, p.3451).
- H1 receptor — cloned 1991 (Yamashita et al.), a 491-amino-acid GPCR; widely expressed on neurons, smooth muscle, epithelium, endothelium and immune cells. Mediates itch, the axon-reflex flare, vasodilation and increased vascular permeability (wheal), bronchoconstriction, and CNS alertness (Wolverton 4e Ch.32, p.350).
- H2 receptor — on gastric parietal cells (acid secretion), plus epithelial/endothelial cells, chondrocytes and immune cells (lymphocytes, neutrophils, eosinophils, monocytes, mast cells, dermal dendritic cells). In skin, H2 contributes (with H1) to vasodilation and increased vascular permeability, and modulates T-lymphocyte activity (Wolverton 4e Ch.32, p.350; Fitzpatrick's 9e Ch.189, p.3457).
- H3 receptor — chiefly a presynaptic autoreceptor on histaminergic neurons (and some immune cells) mediating negative feedback on histamine synthesis and release (Wolverton 4e Ch.32, p.350; Sardana Ch.3).
- H4 receptor — highly expressed in bone marrow and peripheral haematopoietic cells, and on skin mast cells and sensory neurons; implicated in itch (chemotaxis of mast cells/eosinophils). H4-knockout mice and selective H4 agonists/antagonists established its role in pruritus — H4 antagonists reduce the itch of atopic dermatitis experimentally (Wolverton 4e Ch.32, p.350; Fitzpatrick's 9e Ch.189, p.3451; Sardana Ch.3).
- The triple response of Lewis (localised erythema → wheal → surrounding axon-reflex flare) is the classic cutaneous read-out of histamine action and the bedside basis for assaying antihistamine potency (wheal-and-flare suppression) (Wolverton 4e Ch.32, p.350).
- ⚠ Histamine is not the sole mediator of urticarial wheals: up to 50% of chronic urticaria patients do not respond to antihistamines, and CIU wheals last hours (not minutes) — implicating other mediators (PGD2, PAF, cytokines, kinins) and explaining the need for non-antihistamine step-up therapy (Wolverton 4e Ch.32, p.350; Fitzpatrick's 9e Ch.189, p.3453).
3. Mechanism of action — inverse agonism (not simple antagonism)
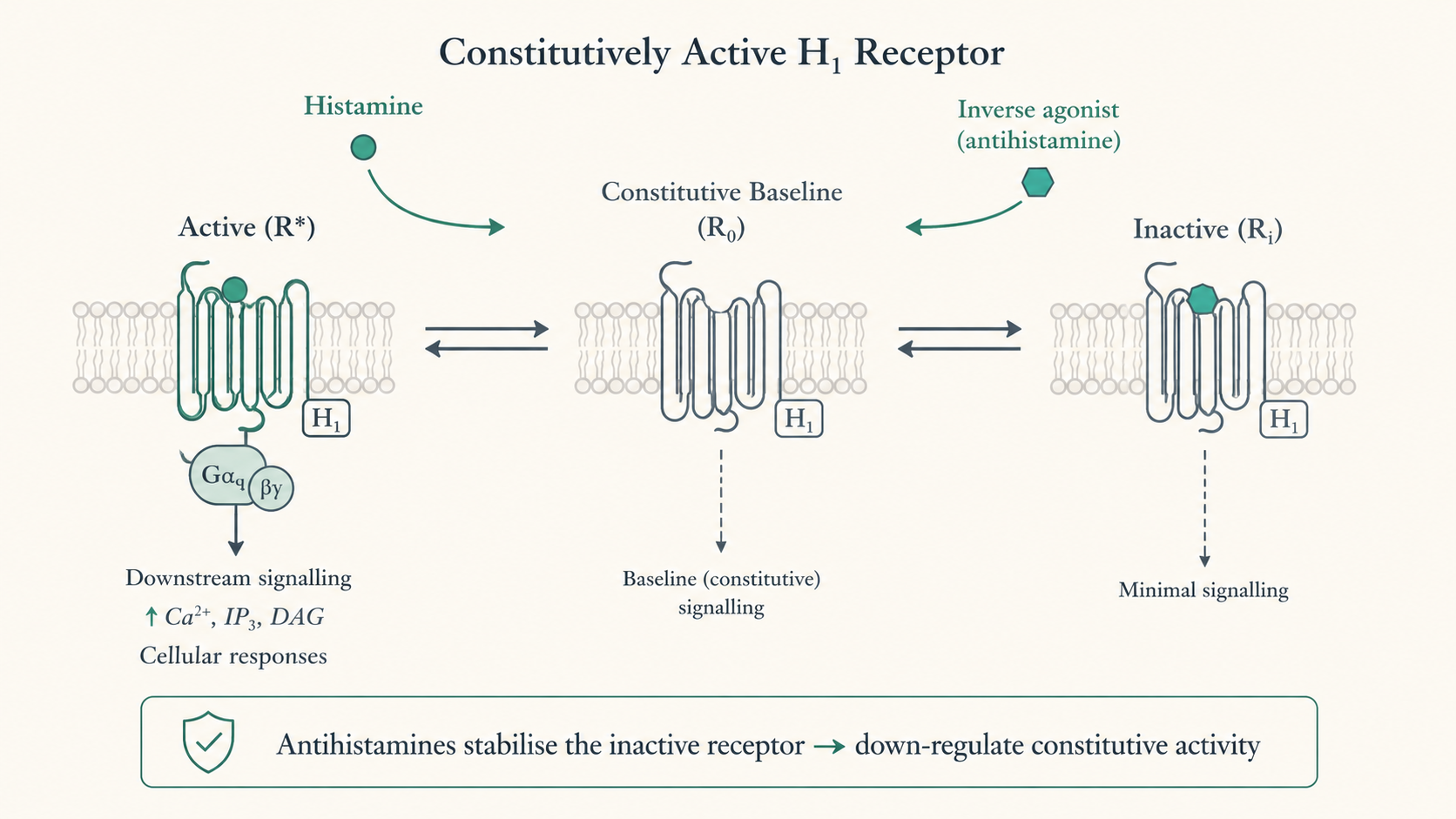
- Key modern concept: H1 and H2 antihistamines are inverse agonists, not classic competitive antagonists. They preferentially bind and stabilise the inactive conformation of the receptor, shifting the constitutive equilibrium toward "off" and thereby down-regulating the constitutively active receptor (Wolverton 4e Ch.32, p.352; Fitzpatrick's 9e Ch.189, p.3451 & Table 189-1).
- Beyond receptor blockade, H1 antihistamines have anti-inflammatory actions via the H1 receptor: ↓ pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-8, GM-CSF), ↓ adhesion-molecule expression (ICAM-1, VCAM-1), ↓ eosinophil/neutrophil chemotaxis, and ↓ release of pre-formed mediators (histamine, PGD2, PAF, tryptase, kinins) — most evident at higher doses (Fitzpatrick's 9e Ch.189, Fig.189-1; Sardana Ch.3).
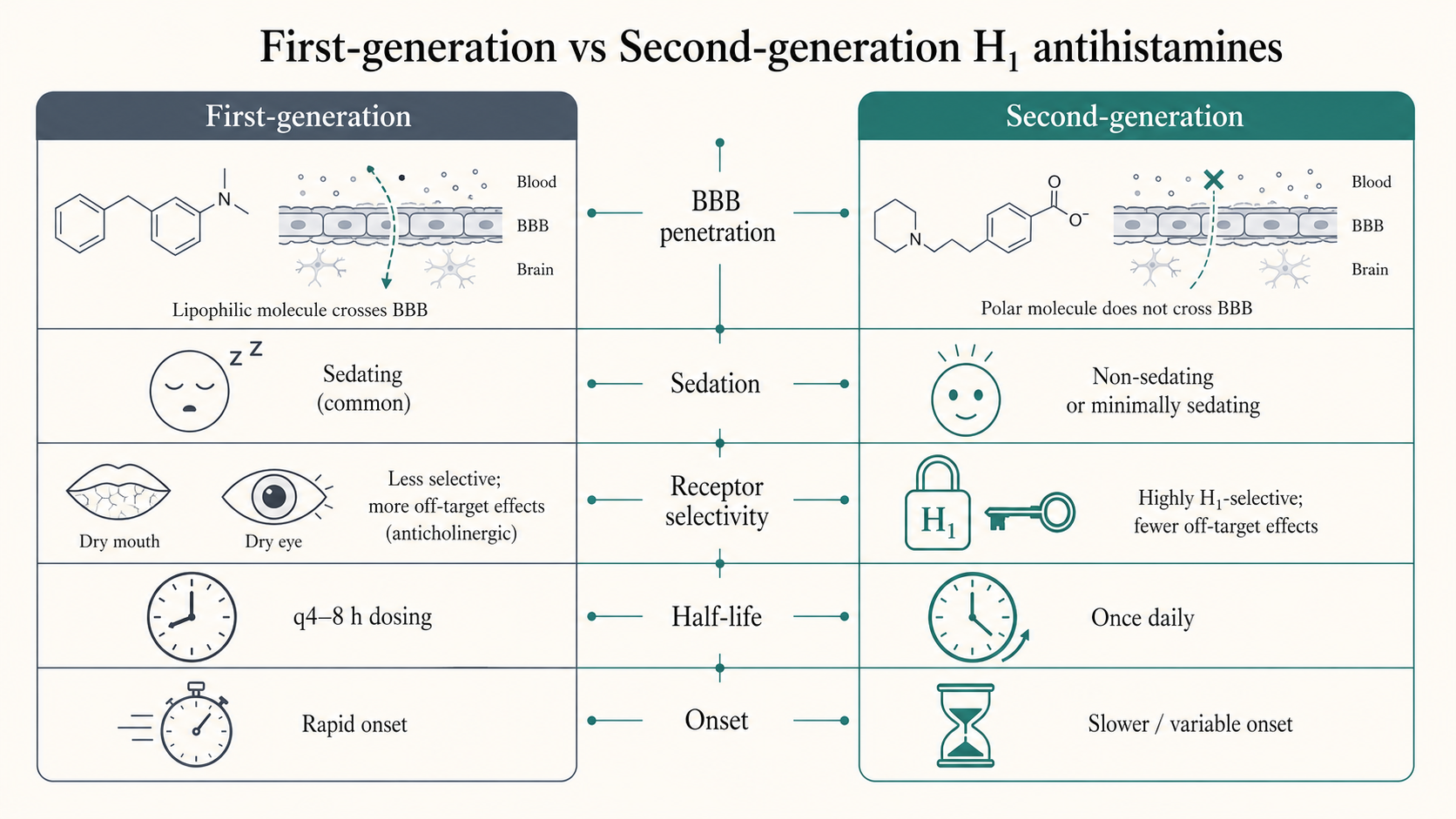
- First-generation agents are lipophilic and cross the blood–brain barrier, blocking the alerting effect of histamine at central H1 receptors → sedation; they are also non-selective, binding muscarinic, α-adrenergic, serotonergic and cardiac ion-channel sites → anticholinergic and cardiac effects (Fitzpatrick's 9e Ch.189, p.3451–3452; Wolverton 4e Ch.32, p.350).
- Second-generation agents are poorly lipophilic, highly H1-selective, and bind noncompetitively / dissociate slowly (longer duration); minimal BBB penetration → little sedation and few anticholinergic effects (Fitzpatrick's 9e Ch.189, p.3452; Wolverton 4e Ch.32, p.352).
- PET imaging with [11C]doxepin showed H1 receptors are densely expressed in cerebral cortex and maintain alertness when activated — the molecular explanation for first-generation sedation and for the "% brain H1 occupancy" metric (e.g. cetirizine occupies ~12% of brain H1 at 10 mg, ~25% at 20 mg) (Wolverton 4e Ch.32, p.350; Fitzpatrick's 9e Ch.189, p.3456).
4. Master classification framework
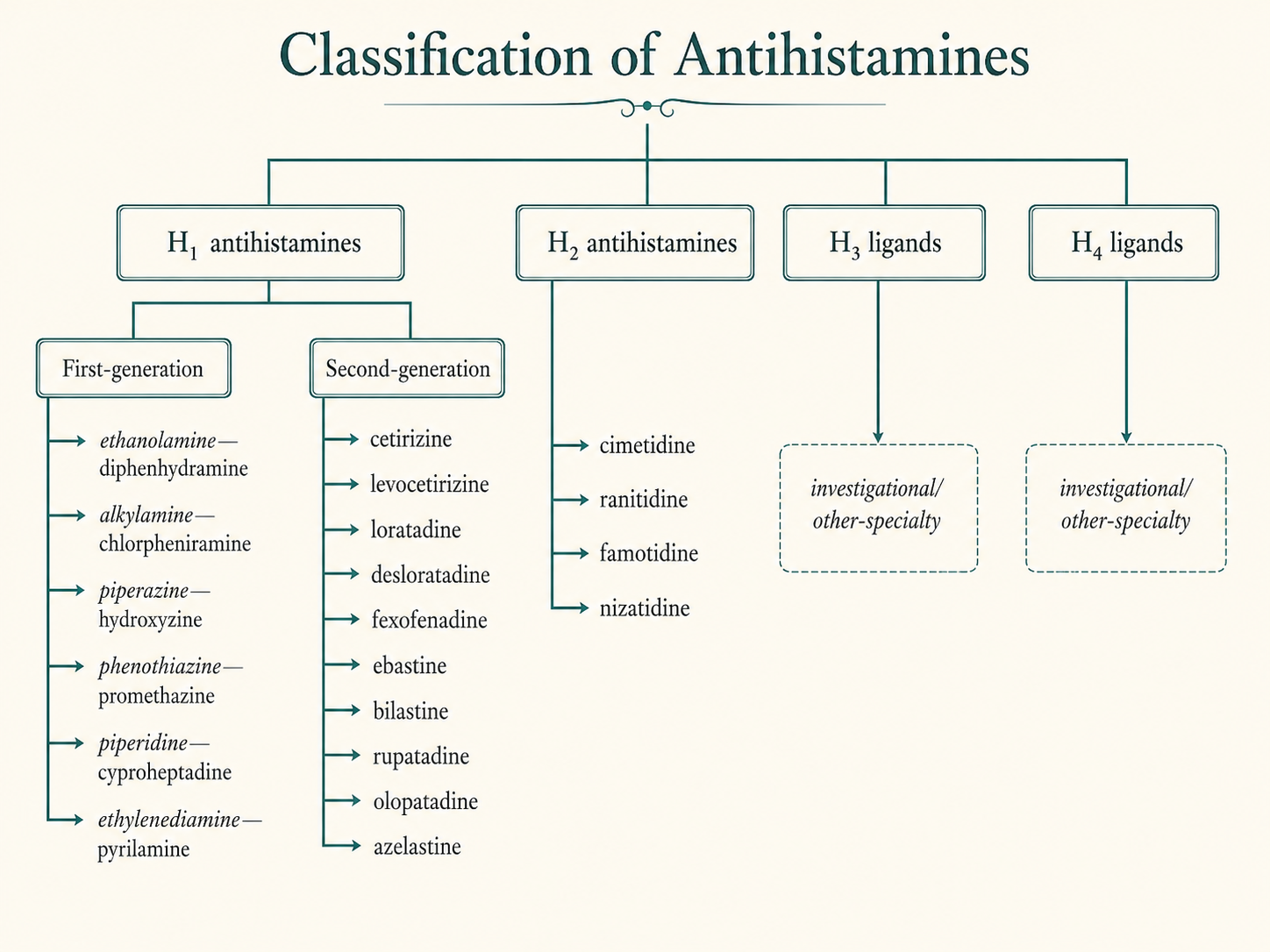
- A. By receptor target
- H1 antihistamines — first-generation, second-generation (± "third-generation" subset).
- H2 antihistamines — cimetidine, ranitidine, famotidine, nizatidine.
- H3 ligands — investigational/other-specialty (autoreceptor antagonists/inverse agonists).
- H4 ligands — investigational antagonists (antipruritic, especially atopic dermatitis).
- (Sardana Ch.3; Wolverton 4e Ch.32, p.350; Fitzpatrick's 9e Ch.189, p.3451)
- B. H1 antihistamines by generation
- First-generation = older, sedating, non-selective, short-acting, multiple daily doses.
- Second-generation = newer, low-/non-sedating, H1-selective, long-acting, once-daily.
- "Third-generation" = a marketing/derivative label for active metabolites and single enantiomers of second-generation drugs (fexofenadine, desloratadine, levocetirizine) — see §7. (Wolverton 4e Ch.32, pp.350–354; Sardana Ch.3)
- C. H1 antihistamines by chemical class (the structure-based classification — most exam-relevant):
- Ethanolamines — diphenhydramine, dimenhydrinate, carbinoxamine, clemastine, doxylamine.
- Ethylenediamines — tripelennamine, antazoline, pyrilamine (mepyramine). (listed by Fitzpatrick's as a distinct 6th group)
- Alkylamines (propylamines) — chlorpheniramine, brompheniramine, dexchlorpheniramine, triprolidine, acrivastine (2nd-gen alkylamine).
- Piperazines — hydroxyzine, cetirizine, levocetirizine, meclizine, cinnarizine, buclizine.
- Piperidines — cyproheptadine, ketotifen, azatadine; loratadine, desloratadine, fexofenadine, ebastine, bilastine, rupatadine, olopatadine (the dominant second-generation class).
- Phenothiazines — promethazine, trimeprazine (alimemazine), methdilazine.
- Phthalazinones — azelastine.
- (Wolverton 4e Ch.32, Table 32.1; Fitzpatrick's 9e Ch.189, p.3451; Sardana Ch.3, Table 3.1)
5. First-generation H1 antihistamines
- Introduced in the 1940s (after Bovet's 1930s work); diphenhydramine, chlorpheniramine and promethazine were the original clinical agents and remained the mainstay until second-generation drugs arrived in the 1980s (Fitzpatrick's 9e Ch.189, p.3451).
- Defining features: lipophilic → cross BBB → sedation; non-selective → anticholinergic (dry mouth, urinary retention, blurred vision, constipation), anti-α-adrenergic (postural hypotension), antiserotonergic and local-anaesthetic actions; short half-life → dosing every 4–8 h; rapid onset (30 min–1 h) (Fitzpatrick's 9e Ch.189, pp.3451–3454; Wolverton 4e Ch.32, p.352).
- Five (Wolverton) / six (Fitzpatrick) chemical subgroups with representative agents:
- Ethanolamine → diphenhydramine (prototype; also dimenhydrinate for vertigo, doxylamine as hypnotic/in pregnancy nausea, clemastine); marked sedation + anticholinergic effect.
- Piperidine → cyproheptadine (also antiserotonergic → used in cold urticaria, appetite stimulation/weight gain, serotonin syndrome).
- Phenothiazine → promethazine (potent, antiemetic, sedative; boxed warning — avoid in children <2 y, respiratory depression; can reverse adrenaline's pressor effect).
- Alkylamine → chlorpheniramine (least sedating of the first-generation group; safe in pregnancy; can cause CNS stimulation — irritability, insomnia, tremor).
- Piperazine → hydroxyzine (strongly antipruritic; prototype for refractory urticaria/anxiety; parent of cetirizine).
- Ethylenediamine → tripelennamine/pyrilamine (Fitzpatrick's distinct group; GI upset prominent).
- (Wolverton 4e Ch.32, Table 32.1 & p.352; Fitzpatrick's 9e Ch.189, p.3451)
- Representative adult doses (examples): diphenhydramine 25–50 mg q4–8h; chlorpheniramine 4 mg TID–QID or 8–12 mg BD (SR); hydroxyzine 25 mg q6–8h (range 10–100 mg); promethazine 12.5–25 mg q6–8h; cyproheptadine 4 mg q8–12h (Wolverton 4e Ch.32, Table 32.2; Fitzpatrick's 9e Ch.189, Table 189-3).
- Cyproheptadine has additional antiserotonin (5-HT) activity — reputedly useful in cold/physical urticaria; causes increased appetite and weight gain via hypothalamic effects; periodic transaminase checks advised (hepatotoxicity reports) (Wolverton 4e Ch.32, p.352; Fitzpatrick's 9e Ch.189, p.3454).
- Caveats: first-generation agents reduce REM sleep (impair next-day memory/attention/psychomotor performance — the "hangover"), increase occupational injuries and road-traffic accidents, and are flagged by the GA2LEN position paper as carrying avoidable risk (Fitzpatrick's 9e Ch.189, pp.3454–3455; Wolverton 4e Ch.32, p.356).
- Contraindications/cautions: narrow-angle glaucoma, prostatic hypertrophy/BPH, concomitant MAO inhibitors, first trimester (traditionally avoided), newborns/premature infants, breastfeeding (1st-gen) (Fitzpatrick's 9e Ch.189, Table 189-4; Wolverton 4e Ch.32, Box 32.1).
6. Second-generation H1 antihistamines
- Developed from the 1980s to remove sedation; low-/non-sedating, H1-selective, long-acting (once-daily), minimal anticholinergic effect — the first-line agents for urticaria and histamine-mediated pruritus (Fitzpatrick's 9e Ch.189, pp.3451–3453; IADVL 5e Ch.37).
- Many are chemically derived from first-generation parents: cetirizine = carboxylic-acid metabolite of hydroxyzine; loratadine is related to azatadine (Fitzpatrick's 9e Ch.189, p.3451; Wolverton 4e Ch.32, p.354).
- Core agents (US set, Wolverton): fexofenadine, loratadine, desloratadine, cetirizine, levocetirizine (Wolverton 4e Ch.32, p.352).
- Worldwide / Indian additions: ebastine, bilastine, rupatadine, mizolastine, acrivastine, azelastine, olopatadine, emedastine, oxatomide — ebastine and olopatadine are widely available in India (Fitzpatrick's 9e Ch.189, p.3453; Sardana Ch.3, Table 3.1).
- Examples with doses: loratadine 10 mg OD; desloratadine 5 mg OD; cetirizine 10 mg OD; levocetirizine 5 mg OD; fexofenadine 120–180 mg OD (or 60 mg BD); ebastine 10–20 mg OD; bilastine 20 mg OD; rupatadine 10 mg OD (Wolverton 4e Ch.32, Table 32.2; Fitzpatrick's 9e Ch.189, Table 189-3; Sardana Ch.3).
- Relative cutaneous potency (wheal-and-flare suppression): cetirizine > fexofenadine > loratadine; levocetirizine (5 mg) and fexofenadine (180 mg) > desloratadine (5 mg) (Fitzpatrick's 9e Ch.189, p.3453).
- Caveat — cetirizine/levocetirizine are the least "non-sedating" of the class: sedation in ~10–15% of users, dose-dependent (because they are piperazines retaining mild BBB penetration); fexofenadine and loratadine/desloratadine are the least likely to enter the brain (essentially no CNS effect) (Fitzpatrick's 9e Ch.189, p.3456; Wolverton 4e Ch.32, p.354).
- No tolerance/tachyphylaxis to first- or second-generation H1 antihistamines on chronic use (placebo-controlled data); a single short-half-life dose can suppress wheal-and-flare for up to 24 h, and regular use prolongs it (6 days of cetirizine → 7 days of suppression) (Fitzpatrick's 9e Ch.189, Table 189-1 & p.3453; Wolverton 4e Ch.32, p.354).
7. The "third-generation" concept (active metabolites & enantiomers)
- A marketing-driven, pharmacologically contested label applied to drugs that are the active metabolite or single enantiomer of a second-generation parent — purportedly cleaner cardiac/CYP profiles (Wolverton 4e Ch.32, pp.352–354; Sardana Ch.3).
- Fexofenadine = active acid metabolite of terfenadine (no liver metabolism; no QT risk) — replaced terfenadine after the latter was withdrawn for torsades de pointes (Wolverton 4e Ch.32, p.354).
- Desloratadine = active metabolite of loratadine (~5× more potent at wheal suppression; not CYP-metabolised) (Wolverton 4e Ch.32, p.354).
- Levocetirizine = the R-enantiomer of cetirizine (the eutomer; ~half the dose at 5 mg, fewer effects) (Wolverton 4e Ch.32, p.354).
- ⚠ Most authorities regard "third-generation" as not a true distinct class — these remain second-generation agents; the term is best used cautiously (Sardana Ch.3; Wolverton 4e Ch.32).
8. Newer / region-specific second-generation agents (extensive examples)
- Bilastine — non-sedating piperidine; not hepatically metabolised, not a CYP substrate, minimal drug interactions; does not cross BBB; 20 mg OD; avoid with food/grapefruit (↓ absorption) (Sardana Ch.3, Table 3.1 & PK table).
- Rupatadine — dual H1 antagonist + PAF (platelet-activating factor) antagonist — theoretical advantage in urticaria where PAF contributes; 10 mg OD (Sardana Ch.3).
- Ebastine — long-acting piperidine; prodrug → active carebastine; 10–20 mg OD; food increases absorption; effective in chronic urticaria and pruritus (Fitzpatrick's 9e Ch.189, p.3453; Sardana Ch.3).
- Olopatadine — H1 antagonist + mast-cell-stabilising activity; rapid oral absorption (~0.5 h); available in India; also topical (ocular/nasal) (Sardana Ch.3).
- Azelastine — phthalazinone; H1 antagonist with mast-cell-stabilising action; mainly topical (nasal spray, eye drops) but oral tablet exists; bitter taste (Fitzpatrick's 9e Ch.189, Table 189-3; Sardana Ch.3).
- Acrivastine — short-acting second-generation alkylamine; rapid onset; in the US only as a fixed combination with pseudoephedrine (Fitzpatrick's 9e Ch.189, Table 189-3).
- Mizolastine, emedastine, oxatomide — additional non-US second-generation agents; emedastine/desloratadine inhibit PAF-induced and TNF-α–induced eosinophil chemotaxis/adhesion in vitro (Fitzpatrick's 9e Ch.189, pp.3452–3453).
- Pharmacogenetics: ~7% of subjects (≈20% of African Americans) are slow metabolisers of desloratadine; P-glycoprotein efflux affects fexofenadine, cetirizine, levocetirizine and mizolastine (relevant to variable bioavailability and CNS exclusion) (Fitzpatrick's 9e Ch.189, p.3453; Sardana Ch.3).
9. Tricyclic antidepressants with antihistamine activity
- Doxepin — tricyclic antidepressant that is a potent dual H1 + H2 antagonist; ~800× more potent than diphenhydramine at the H1 receptor (Wolverton 4e Ch.32, p.356; Fitzpatrick's 9e Ch.189, p.3459).
- Uses: refractory chronic urticaria, physical urticarias, and chronic pruritus (incl. AD, lichen simplex chronicus); especially useful when urticaria coexists with anxiety/depression; oral 10–75 mg at night (start 10 mg) (Wolverton 4e Ch.32, pp.356–357; Fitzpatrick's 9e Ch.189, p.3459).
- Topical doxepin 5% cream — antipruritic for AD/LSC; main adverse effects sedation and allergic contact dermatitis (Fitzpatrick's 9e Ch.189, p.3459).
- Cautions: anticholinergic effects, raised intra-ocular pressure (avoid in glaucoma), do not combine with MAOIs, monitor for suicidal ideation; oral = pregnancy category C, topical = category B; contraindicated in breastfeeding; not for children <12 y (Wolverton 4e Ch.32, p.356; Fitzpatrick's 9e Ch.189, p.3459).
- Mirtazapine — tetracyclic antidepressant with significant H1 antihistamine activity (plus 5-HT2/5-HT3 binding) — reported for chronic pruritus (Wolverton 4e Ch.32, p.356).
10. Antihistamines with mast-cell-stabilising activity
- Ketotifen — benzocycloheptathiophene; H1 antihistamine + mast-cell/basophil stabiliser; used in physical urticarias, CIU and mastocytosis; relieved pruritus better than clemastine/placebo in CIU; sedative + atropine-like effects; in the US available only as an ophthalmic solution (Fitzpatrick's 9e Ch.189, p.3459; Wolverton 4e Ch.32, p.350).
- Olopatadine, azelastine — dual H1-antagonist/mast-cell-stabilising agents (see §8).
- ⚠ The mast-cell-stabilising claim of ketotifen is not fully substantiated — it does not significantly lower urinary histamine metabolites in urticaria/mastocytosis, questioning true membrane stabilisation (Wolverton 4e Ch.32, p.350).
- Cromolyn (sodium cromoglicate) — a pure mast-cell stabiliser (not an H1 antihistamine) listed alongside for completeness; poor oral absorption (~1%); used in systemic mastocytosis GI symptoms (Wolverton 4e Ch.32, Table 32.2).
11. H2 antihistamines
- Agents: cimetidine, ranitidine, famotidine, nizatidine — selective inverse agonists at H2 receptors (Fitzpatrick's 9e Ch.189, p.3457; Wolverton 4e Ch.32, p.355).
- Primary use is acid-peptic disease (parietal-cell H2 blockade), but in dermatology they are second/third-line adjuncts: combined with an H1 antihistamine in refractory CIU/angioedema, in acute allergic reactions/anaphylaxis adjunct, and for GI symptoms of mastocytosis (Fitzpatrick's 9e Ch.189, Table 189-6; Wolverton 4e Ch.32, p.357).
- Modest skin benefit: adding H2 to H1 reduces wheal-and-flare by only a further 5–15%; cutaneous H2-receptor expression is low — part of the apparent benefit of adding cimetidine is pharmacokinetic (it raises H1-antihistamine plasma levels by inhibiting their metabolism) rather than true H2 blockade; guidelines rate combined H1+H2 as weak, third-line (Wolverton 4e Ch.32, p.357; Fitzpatrick's 9e Ch.189, p.3457).
- PK: rapidly absorbed (peak 1–2 h), mostly renal excretion unchanged (10–35% hepatic), limited BBB penetration; cimetidine t½ ~2 h, ranitidine 2–3 h, famotidine 3–8 h (>20 h in renal failure), nizatidine 1–2 h (Fitzpatrick's 9e Ch.189, p.3457).
- Cimetidine-specific adverse effects: antiandrogenic — gynaecomastia, galactorrhoea (↑ prolactin), ↓ libido, impotence, ↓ sperm counts (esp. >1600 mg/day); strongest CYP inhibitor of the class → many interactions (warfarin, phenytoin, theophylline, β-blockers, benzodiazepines, CCBs, SSRIs, metformin) — contraindicated with dofetilide (QT/torsades). Ranitidine is the preferred H2 agent when interactions matter (less CYP inhibition); famotidine/nizatidine have the fewest interactions (Wolverton 4e Ch.32, p.355; Fitzpatrick's 9e Ch.189, pp.3458–3459).
- Note: cimetidine's old anecdotal use for viral warts (T-cell immunomodulation via H2) was not confirmed in randomised trials (Wolverton 4e Ch.32, p.350).
12. H3 and H4 ligands (receptor pharmacology)
- H3 receptor — presynaptic autoreceptor on histaminergic neurons; antagonists/inverse agonists increase central histamine release, underlying CNS/wakefulness applications. Standard dermatology texts characterise the receptor and a local antagonist effect, but no H3-selective agent has an established routine dermatological indication (Wolverton 4e Ch.32, p.350; Sardana Ch.3).
- H4 receptor — on mast cells, eosinophils and sensory neurons; central to itch. H4-receptor antagonists are superior to traditional antihistamines at attenuating experimental pruritus and reduce the itch of atopic dermatitis in models — the rationale for H4-targeted antipruritics (Wolverton 4e Ch.32, p.350 & ref. Dunford 2007; Sardana Ch.3).
13. Pharmacokinetics — comparative
- First-generation: onset 30 min–1 h; hepatic CYP3A4 metabolism (glucuronidation) → renal excretion; many also inhibit CYP2D6; short half-life but tissue persistence can give >plasma-half-life duration; some (brompheniramine, chlorpheniramine, hydroxyzine) have serum half-lives >20 h despite short clinical action (Fitzpatrick's 9e Ch.189, pp.3453–3454; Wolverton 4e Ch.32, p.352).
- Second-generation — two metabolic patterns:
- CYP3A4-metabolised (loratadine, ebastine, mizolastine, acrivastine, oxatomide) → susceptible to interaction with macrolides/azoles (historically dangerous with terfenadine/astemizole).
- Minimally metabolised / renally cleared (cetirizine, levocetirizine, fexofenadine, desloratadine) → few CYP interactions; adjust dose in renal impairment (Fitzpatrick's 9e Ch.189, p.3453; Sardana Ch.3).
- Examples: cetirizine/levocetirizine peak ~1 h, t½ 6.5–10 h, mostly renal unchanged; fexofenadine peak 2–3 h, t½ ~14 h, ~80% faecal, no hepatic metabolism (no dose change in liver disease); desloratadine t½ 19–34 h (Wolverton 4e Ch.32, Table 32.3; Fitzpatrick's 9e Ch.189, p.3453).
- Absorption pearls: fexofenadine absorption reduced by antacids and is a P-gp substrate; food increases ebastine/loratadine absorption; grapefruit/orange/apple juice reduce fexofenadine bioavailability (Fitzpatrick's 9e Ch.189, p.3454; Sardana Ch.3).
14. Adverse effects
- First-generation (class effects): sedation (greatest with ethanolamines & phenothiazines, least with alkylamines), impaired psychomotor/cognitive performance, paradoxical CNS stimulation in children (excitation, insomnia, tremor, even convulsions/hallucinations in overdose); anticholinergic (dry mucosae, urinary retention, blurred vision, constipation, erectile dysfunction); postural hypotension; weight gain (cyproheptadine); rare cardiac (QT) (Fitzpatrick's 9e Ch.189, Table 189-5; Wolverton 4e Ch.32).
- Second-generation: generally well tolerated — minimal sedation (except cetirizine/levocetirizine ~10–15%), few anticholinergic effects; rare GI upset, headache (Fitzpatrick's 9e Ch.189, p.3456).
- Cardiotoxicity — historical lesson: terfenadine and astemizole were withdrawn worldwide for QT prolongation and torsades de pointes (blockade of cardiac K+/IKr channels, especially with CYP3A4 inhibitors); current second-generation agents have ~1000-fold lower cardiac-channel affinity and are considered cardiac-safe (Fitzpatrick's 9e Ch.189, p.3456; Wolverton 4e Ch.32, p.354).
- H2 antihistamines: generally safe; CNS (confusion/headache/dizziness, esp. elderly/renal disease), rare thrombocytopenia/granulocytopenia, cimetidine antiandrogen effects, masking of gastric carcinoma; necrotising enterocolitis risk in neonates (Fitzpatrick's 9e Ch.189, Table 189-8).
- Cutaneous reactions to oral H1 antihistamines are rare (eczematous/allergic contact dermatitis, urticaria, fixed drug eruption, photosensitivity — sometimes excipient-related); topical H1 antihistamines carry a notable risk of allergic contact dermatitis (Fitzpatrick's 9e Ch.189, pp.3453, 3456).
15. Drug interactions
- First-generation H1: additive CNS depression with alcohol, benzodiazepines, opioids; contraindicated with MAOIs (prolong anticholinergic/sedative effect); inhibit CYP2D6 (↑ metoprolol, venlafaxine); phenothiazines can reverse adrenaline's pressor effect (use noradrenaline/phenylephrine) (Fitzpatrick's 9e Ch.189, p.3456; Wolverton 4e Ch.32, Table 32.4).
- Second-generation H1: CYP3A4-metabolised agents interact with macrolides/azoles (clinically minor for current agents); fexofenadine ↓ by antacids (Fitzpatrick's 9e Ch.189, p.3453).
- H2 (cimetidine): broad CYP inhibition (2D6/1A2/2C19/3A4) → ↑ warfarin, theophylline, phenytoin, statins, ciclosporin, benzodiazepines, β-blockers, CCBs, metformin, SSRIs; contraindicated with dofetilide; cimetidine/ranitidine inhibit alcohol dehydrogenase (↑ blood alcohol) (Wolverton 4e Ch.32, Table 32.5; Fitzpatrick's 9e Ch.189, pp.3458–3459).
16. Special populations
- Pregnancy: no firm evidence of teratogenicity; preferred first-generation = chlorpheniramine, diphenhydramine (most data, category B); preferred second-generation = cetirizine, loratadine (category B). Avoid in first trimester where possible; a meta-analysis of 200,000 first-trimester exposures showed no increase in malformations (Wolverton 4e Ch.32, p.355; Fitzpatrick's 9e Ch.189, pp.3456–3457; IADVL 5e Ch.37).
- Lactation: cetirizine and loratadine excreted in low amounts → preferred; first-generation agents may reduce milk supply (anticholinergic) and sedate the infant (Wolverton 4e Ch.32, p.355).
- Children: avoid sedating first-generation agents where possible (paradoxical excitation, poisoning risk); cetirizine, levocetirizine, loratadine well studied from 6–36 months; up-dosing safety data limited in paediatrics (Fitzpatrick's 9e Ch.189, p.3456; IADVL 5e Ch.37).
- Elderly: caution with first-generation agents (anticholinergic load — urinary retention, constipation, hypotension, confusion, falls); H2 CNS effects more likely (Fitzpatrick's 9e Ch.189, p.3456).
- Renal/hepatic impairment: reduce dose of renally cleared agents (cetirizine, levocetirizine — both renal+hepatic adjustment) in renal disease; fexofenadine needs no hepatic adjustment; H2 agents need renal dose reduction (Fitzpatrick's 9e Ch.189, Table 189-3; Wolverton 4e Ch.32, p.354).
17. Therapeutic role in dermatology
- Chronic spontaneous (idiopathic) urticaria (CSU/CIU): second-generation non-sedating H1 antihistamines are the cornerstone, first-line therapy; effective in ~50%; updosing and step-up for the rest (Wolverton 4e Ch.32, p.356; IADVL 5e Ch.37; Fitzpatrick's 9e Ch.189, p.3453).
- Physical/inducible urticarias (dermographism, cholinergic, cold, delayed-pressure): H1 antihistamines are mainstay; cyproheptadine traditionally favoured for cold urticaria (Wolverton 4e Ch.32, p.356).
- Pruritus: useful where itch is histamine-mediated (urticaria, mastocytosis, insect bites); first-generation agents help nocturnal itch mainly via sedation (Fitzpatrick's 9e Ch.189, p.3453; IADVL 5e Ch.96 Antipruritic Agents).
- Atopic dermatitis: evidence for antihistamines is weak/ambiguous — benefit is largely the soporific effect of first-generation agents on night-time scratching, not true antipruritic action; the AAD (2014) discourages routine use; reserve for AD patients with concomitant urticaria/allergic rhinitis (Wolverton 4e Ch.32, p.357; Fitzpatrick's 9e Ch.189, p.3453).
- Mastocytosis: H1 (often updosed, e.g. fexofenadine 360 mg AM + cetirizine 40 mg PM) ± H2 for GI/flushing symptoms (Fitzpatrick's 9e Ch.189, pp.3453–3457).
- Anaphylaxis: antihistamines are adjuncts only — adrenaline is first-line; H1 ± H2 for cutaneous symptoms (IADVL 5e Ch.37; Fitzpatrick's 9e Ch.189, Table 189-6).
18. Dosing, up-dosing & the urticaria treatment ladder
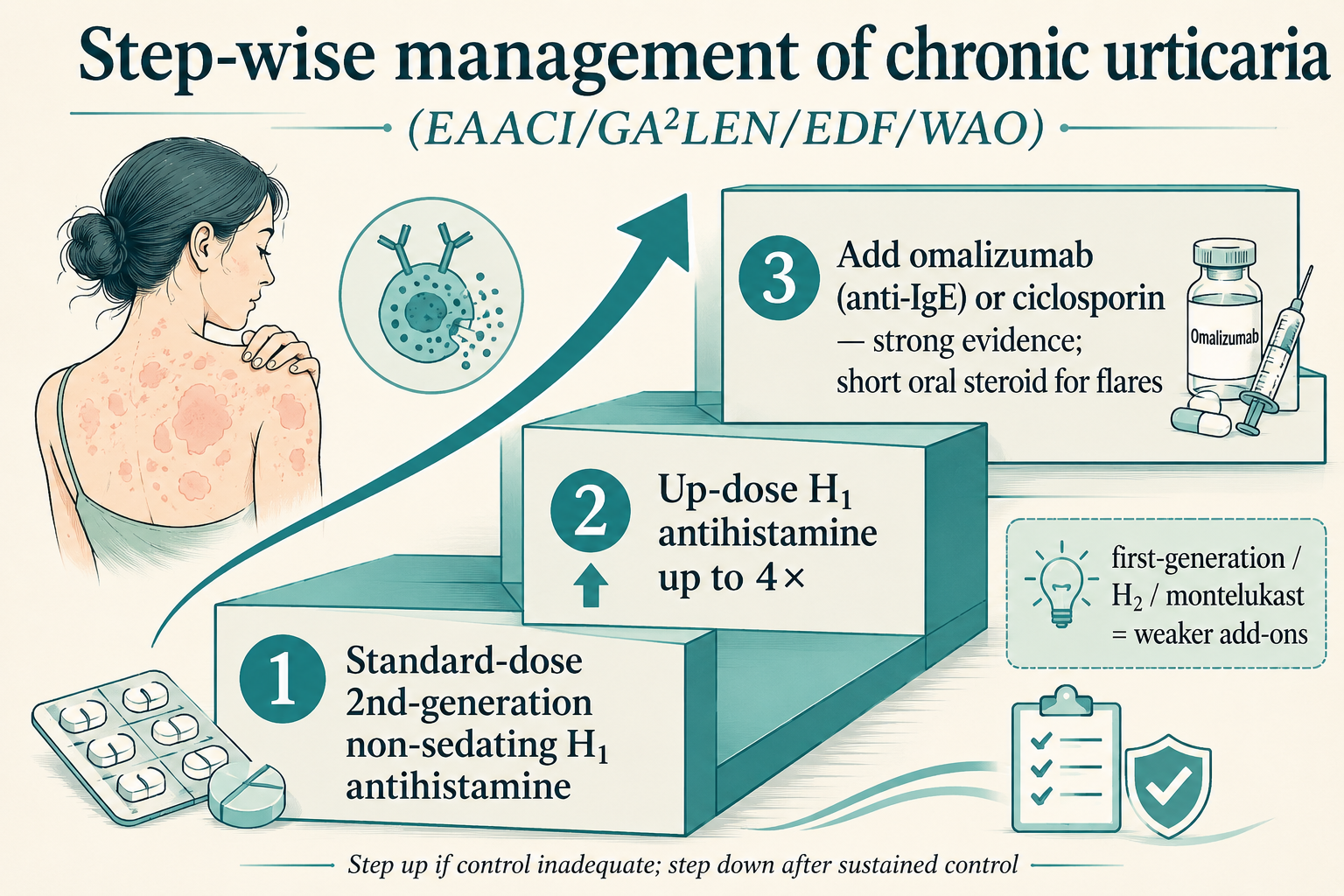
- EAACI/GA2LEN/EDF/WAO step-wise algorithm (as carried in IADVL 5e Ch.37, Step-wise management of chronic urticaria, Fig. 37.4):
- Step 1 — standard-dose second-generation non-sedating H1 antihistamine.
- Step 2 — if inadequate after ~2–4 weeks, increase the dose up to 4× (fourfold) the standard (off-label but guideline-endorsed); may rotate/switch agent or combine.
- Step 3 — if still refractory, add omalizumab (anti-IgE) or ciclosporin (3–5 mg/kg/day) — strong evidence; a short course of oral corticosteroid for severe exacerbations; consider adding a first-generation sedating antihistamine (e.g. hydroxyzine) at night or an H2 antagonist or montelukast as weaker add-ons.
- (IADVL 5e Ch.37, Fig. 37.4)
- Up-dosing evidence: fourfold dosing of fexofenadine/desloratadine/loratadine significantly improves pruritus and wheal-and-flare in resistant CSU vs standard dose (Godse; Staevska) — at the cost of more potential sedation; preferred to combining different antihistamines (Wolverton 4e Ch.32, p.356; IADVL 5e Ch.37 refs 22–23).
- Practical refractory regimen (Wolverton authors): fexofenadine 180–360 mg AM + cetirizine 10–40 mg PM; substitute doxepin 10–75 mg at night where anxiety/depression coexists (Wolverton 4e Ch.32, pp.356–357).
- Omalizumab (anti-IgE mAb) — for antihistamine-refractory CSU, 150–300 mg SC every 4 weeks; observe ~2 h post-dose (anaphylaxis risk); strong-evidence step-3 agent (IADVL 5e Ch.37; Wolverton 4e Ch.31 — Dupilumab, Omalizumab, Others).
19. Topical antihistamines
- Topical H1 formulations (e.g. diphenhydramine, doxepin 5% cream) exist for localised pruritus but are less effective than systemic agents and carry a real risk of allergic contact dermatitis with prolonged/widespread use — generally discouraged (Fitzpatrick's 9e Ch.189, p.3453; Wolverton 4e Ch.32, p.356).
- Topical/ocular/nasal mast-cell-stabilising antihistamines — azelastine, olopatadine, ketotifen, emedastine — are mainstays for allergic conjunctivitis/rhinitis (Fitzpatrick's 9e Ch.189; Sardana Ch.3).
20. High-yield comparisons & exam pearls
- First- vs second-generation (one-line discriminators): lipophilic vs hydrophilic; sedating vs non-sedating; non-selective (anticholinergic) vs H1-selective; short-acting (q4–8h) vs long-acting (OD); rapid onset vs slower; cheap/old vs newer (Fitzpatrick's 9e Ch.189, Table 189-1).
- Prototype drugs to name: diphenhydramine (ethanolamine), chlorpheniramine (alkylamine), hydroxyzine (piperazine, parent of cetirizine), promethazine (phenothiazine), cyproheptadine (piperidine, antiserotonin), doxepin (TCA, dual H1/H2, 800× diphenhydramine), ketotifen (mast-cell stabiliser).
- Metabolite/enantiomer chains: hydroxyzine→cetirizine→(R-enantiomer) levocetirizine; loratadine→desloratadine; terfenadine→fexofenadine (Wolverton 4e Ch.32, p.354).
- Withdrawn for cardiotoxicity: terfenadine, astemizole (torsades) (Fitzpatrick's 9e Ch.189, p.3456).
- Mechanism buzzword: antihistamines are inverse agonists stabilising the inactive receptor (Fitzpatrick's 9e Ch.189, Table 189-1).
- Urticaria ladder buzz: 2nd-gen → 4× updose → omalizumab/ciclosporin (IADVL 5e Ch.37, Fig. 37.4).
- Dual-action newer agents: rupatadine (H1 + PAF), olopatadine/azelastine/ketotifen (H1 + mast-cell stabiliser), bilastine (no CYP, no food) (Sardana Ch.3).
RECENT ADVANCES
Recent Advances updated on 20 Jun 2026 — sources: PubMed, US-FDA, CDSCO/DCGI, manufacturer press releases (Sanofi/Regeneron, Novartis), EAACI/GA2LEN/EuroGuiDerm/APAAACI.
The "classification of antihistamines" frontier in 2026 has moved beyond the H1/H2 axis in two directions — (i) new receptor-targeted antihistamine classes (H3 ligands, H4 antagonists), and (ii) histamine-pathway-directed biologics/small molecules that supersede antihistamines in refractory disease (anti-IL-4Rα, BTK inhibitors, anti-KIT).
RA 1. New Approvals & Label Expansions (beyond H1/H2)
![Figure 6 [RA] — Beyond H1 H2 landscape](images/classification-of-antihistamines/derma_classification-of-antihistamines_ra_01_beyond-h1-h2-landscape.png)
- Dupilumab (Dupixent, anti-IL-4Rα) — FDA approved April 2025 for chronic spontaneous urticaria (CSU) in adults and adolescents ≥12 years who remain symptomatic on H1-antihistamines — the first new targeted CSU therapy in over a decade [FDA 2025-Apr].
- Dupilumab — FDA paediatric expansion April 2026 to children aged 2–11 years with CSU persisting despite H1-antihistamines; injection-site reactions were the commonest adverse event with no new safety signals [FDA 2026-Apr].
- Remibrutinib (Rhapsido, oral BTK inhibitor) — FDA first approval 30 Sep 2025 for CSU in adults symptomatic despite H1-antihistamine treatment; subsequently approved in China, under EU/Japan review. According to PubMed; DOI.
- Bruton tyrosine kinase (BTK) has emerged as a validated mast-cell/basophil signalling target in allergic skin disease, blocking the FcεRI→BTK cascade upstream of histamine release. According to PubMed; DOI
RA 2. Emerging Receptor Targets — H3 and H4 Ligands
- H4-receptor antagonists — clinical development history: the first selective H4R antagonist JNJ-7777120 was a pivotal pharmacological tool establishing the H4R role in inflammation and pruritus, but a short in-vivo half-life and rat/dog hypoadrenocorticism toxicity blocked clinical translation. According to PubMed; DOI.
- JNJ-39758979 (selective H4R antagonist) showed efficacy in experimental pruritus and in atopic-dermatitis patients, but development was terminated due to drug-induced agranulocytosis. According to PubMed; DOI
- Toreforant — a chemically distinct H4R antagonist without the agranulocytosis liability — has been tested in rheumatoid arthritis, asthma and psoriasis; clinical data overall suggest H4R antagonists can benefit atopic dermatitis and pruritus. According to PubMed; DOI
- Adriforant (ZPL-3893787) — an oral H4R antagonist evaluated in atopic dermatitis — is the other clinical-stage H4 agent named in the patent/ligand literature. According to PubMed; DOI
- Mechanistic update (2024): the H4R, acting with TRPV1 and PLC, mediates itch evoked by cadaverine (a gut-microbiome metabolite) — reinforcing H4R as an antipruritic target distinct from the histamine→H1 itch axis. According to PubMed; DOI
- Histamine-receptor pharmacology of allergic skin disease now frames H1 (itch/flare), H2 (minor cutaneous role), and H4 (mast-cell/eosinophil chemotaxis, itch) as complementary antihistamine targets. According to PubMed; DOI and DOI
- H3 ligand — pitolisant: the approved H3-receptor inverse agonist/antagonist is indicated for narcolepsy/excessive daytime sleepiness, exploiting H3-autoreceptor blockade to raise central histamine and wakefulness — it has no dermatological indication (the only marketed H3 drug; betahistine remains the H1-analogue used for Ménière's). According to PubMed; DOI and DOI
RA 3. Landmark Trials & Meta-Analyses
- LIBERTY-CSU CUPID-A & CUPID-C (2025): replicate phase 3 RCTs of dupilumab vs placebo in anti-IgE-naïve CSU uncontrolled on H1-antihistamines significantly reduced itch and hive severity over 24 weeks, supporting the FDA approval. According to PubMed; DOI.
- Barzolvolimab (anti-KIT mAb) — phase 1b CSU (2025): mast-cell-depleting therapy gave rapid (within 1 week) and sustained symptom control in antihistamine-refractory CSU — 71% achieved well-controlled disease (UAS7 ≤6) and 57% a complete response (UAS7 = 0) by week 12; hair-colour change was the commonest adverse event. According to PubMed; DOI
- Bilastine — systematic review & meta-analysis (2022): 7 RCTs / 975 chronic-urticaria patients; bilastine significantly improved dermatology quality-of-life index and Total Symptom Score vs control. According to PubMed; DOI.
- Bilastine vs levocetirizine — phase 3 non-inferiority RCT (2024): multicentre double-blind trial in chronic idiopathic urticaria showed bilastine non-inferior to levocetirizine. According to PubMed; DOI
- Emerging IgE- and non-IgE-targeted therapies for chronic urticaria (2025 review): maps the pipeline (anti-IgE ligelizumab, IL-4/13 dupilumab, BTK inhibitors, anti-KIT) succeeding antihistamines in refractory disease. According to PubMed; DOI
RA 4. Combination, Sequential & Updosing Therapies
- H1-antihistamine up-dosing — rupatadine RCT (2023): on-demand vs daily rupatadine in CSU with a randomised updosing arm (10→20 mg) confirmed the value of updosing and explored disease-modifying effects of continuous dosing. According to PubMed; DOI.
- Switching antihistamine — H1-SWITCH trial (2024): switching refractory-CSU patients to bilastine improved control in an open-label randomised comparative study, supporting agent-switching as a practical step before biologics. According to PubMed; DOI
- Rupatadine global safety evaluation (2016): pooled allergic-rhinitis/urticaria data confirmed a favourable cardiac/CNS safety profile for the dual H1/PAF antagonist. According to PubMed; DOI
RA 5. Major Guideline Updates
- International EAACI/GA2LEN/EuroGuiDerm/APAAACI urticaria guideline (Zuberbier et al, Allergy 2022): reaffirms second-generation non-sedating H1-antihistamines as first-line; does NOT recommend first-generation (sedating) antihistamines for routine chronic-urticaria management; second-line = up-dose the same SGA up to 4×; third-line = add omalizumab, then ciclosporin — on the basis of good efficacy, good safety and low cost. According to PubMed; DOI.
RA 6. Indian Regulatory & Society Actions
- Bilastine — DCGI/CDSCO approval (India): the non-sedating SGA (20 mg) is approved and marketed in India for allergic rhinitis and urticaria [DCGI].
- Bilastine 20 mg + montelukast 10 mg — fixed-dose combination approved by CDSCO for allergic rhinitis in adults [CDSCO] (note: antihistamine-with-bronchodilator and multi-antihistamine FDCs are banned in India — the montelukast FDC is a separately-sanctioned combination, not in those banned categories).
- Modern Indian SGA armamentarium now routinely includes bilastine, rupatadine, ebastine, olopatadine, fexofenadine, levocetirizine, desloratadine — the second-generation roster is fully available in India.
![Figure 7 [RA] — Updated CSU ladder](images/classification-of-antihistamines/derma_classification-of-antihistamines_ra_02_updated-csu-ladder.png)
Multi-source disagreements
- ⚠ Number of first-generation chemical classes: Fitzpatrick's 9e (Ch.189, p.3451) divides first-generation H1 agents into 6 groups (ethylenediamines, ethanolamines, alkylamines, phenothiazines, piperazines, piperidines), whereas Wolverton 4e (Ch.32, Table 32.1) lists 5 representative classes (omits ethylenediamine, using ethanolamine/piperidine/phenothiazine/alkylamine/piperazine). Reason: Wolverton tabulates the clinically dominant US agents; the ethylenediamines (tripelennamine, antazoline, pyrilamine) are an older, less-used group still counted by Fitzpatrick's. Sardana Ch.3 adds phthalazinones (azelastine) as a further chemical class — so the full structural list is ≥7 groups.
- ⚠ "Third-generation" antihistamines: treated as a useful descriptor by some (active metabolites/enantiomers with cleaner profiles) but explicitly considered not a genuine separate class by Sardana/Wolverton; both descriptors remain in use.
- ⚠ H2 antihistamines in urticaria: Fitzpatrick's lists H2 as a useful adjunct in refractory CIU, while Wolverton stresses the benefit is largely pharmacokinetic (cimetidine raising H1 levels) and rates combined H1+H2 as weak/third-line — best regarded as a weak, largely PK-mediated adjunct.
- ⚠ Ketotifen mast-cell stabilisation: asserted (Fitzpatrick's) vs questioned (Wolverton — no fall in urinary histamine metabolites).