Peptic Ulcer Disease — Anti-ulcer Drugs, H. pylori & GERD
Acid-suppressants, mucosal protectives, H. pylori eradication & reflux therapy — mechanism, choice & recent advances
Past RGUHS + DNB + MPMSU + MUHS + VNSGU · 34
RGUHSSep '25
RGUHSMay '25
MPMSUOct '25
DNBDec '25
VNSGUSep '25
RGUHSDec '23
RGUHSJul '23
MUHSSummer '23
RGUHSMay '22
MUHSWinter '21
RGUHSNov '20
RGUHSJun '20
MUHSSummer '20
RGUHSMay '19
RGUHSNov '18
MPMSU2018
MUHSSummer '18
MPMSU2017
MUHSSummer '17 Suppl
DNBDec '15
DNBDec '14
MPMSU2012
DNBDec '12
DNBDec '12
RGUHSMay '11
MPMSU2011
RGUHSOct '10
MPMSU2010
RGUHSMay '09
RGUHSMay '09
MPMSU2009
RGUHSSep '07
MPMSU2005
MPMSU1993
Introduction & pathophysiology
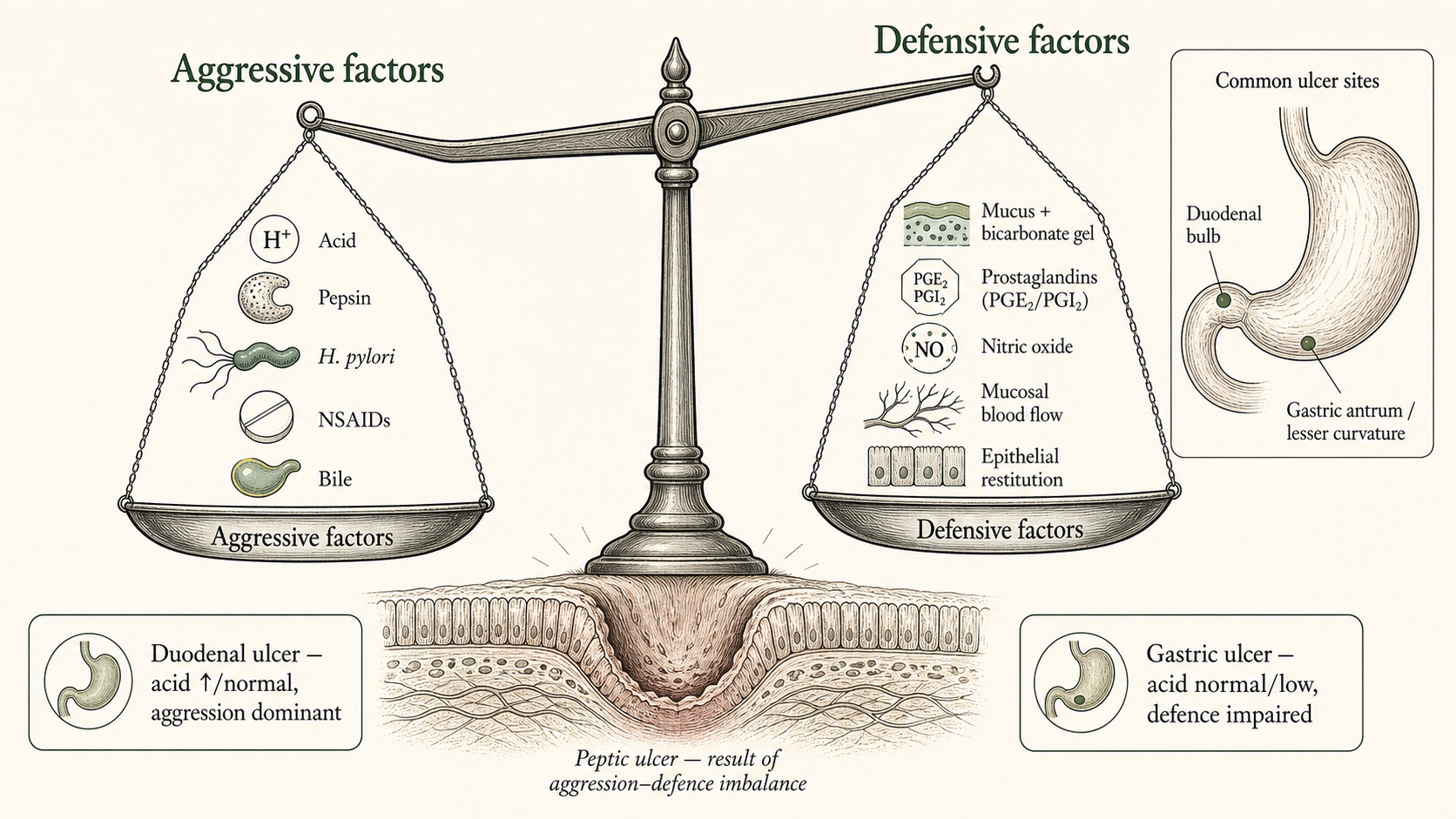
- Acid-peptic disorders — comprise GERD, peptic ulcer disease (PUD) (gastric + duodenal) and stress-related mucosal injury; mucosal ulceration arises when aggressive factors (acid, pepsin, NSAIDs, H. pylori, bile) overwhelm defensive factors (mucus–bicarbonate, prostaglandins, NO, mucosal blood flow, restitution).
- Peptic ulcer — a mucosal break ≥5 mm penetrating the muscularis mucosae, in the acid-/pepsin-exposed stomach and duodenum — deeper than an erosion.
- Two-pronged therapeutic logic — (a) reduce gastric acidity (antacids, H2 antagonists, PPIs, P-CABs) and (b) enhance mucosal defence (misoprostol, sucralfate, bismuth); GERD adds a third lever — raising LES tone / improving motility.
- Central paradigm shift — recognising H. pylori as the cause of most ulcers turned a chronically relapsing disease into a curable one through eradication — >90% of peptic ulcers are caused by H. pylori or NSAIDs/aspirin.
- DU vs GU pathophysiology — duodenal ulcer — acid high or normal (basal/nocturnal hypersecretion), acid-dominant; gastric ulcer — acid normal/low, impaired mucosal defence predominates; but "no acid, no ulcer" holds for both.
- H. pylori mechanism — spiral microaerophilic gram-negative rod; high urease generates ammonia for acid survival; antral-predominant gastritis ↓somatostatin → hypergastrinaemia → DU; corpus gastritis → GU, atrophy and cancer (WHO class-I carcinogen — chronic gastritis, PUD, MALT lymphoma, adenocarcinoma).
- NSAID mechanism — mainly systemic — COX-1 inhibition suppresses protective PGE2/PGI2; risk is additive with low-dose aspirin, corticosteroids, anticoagulants (GI-bleed up to ~20× with warfarin) and co-existing H. pylori; COX-2-selective agents spare GI toxicity.
Continue reading
Peptic Ulcer Disease
PharmaNotes Pro · LAQ
Sign in with your Google account. If you're already subscribed, the chapter unlocks immediately — otherwise, pick Monthly or Annual on the next step.