Drug Dosage Principles & Individualisation
Loading, maintenance, special populations and genotype-guided precision dosing
Past RGUHS + DNB + MPMSU + MUHS · 107
RGUHSSep '25
DNBDec '25
DNBDec '25
DNBDec '25
MUHSWinter '25
MPMSUJan '25
MPMSUMay '25
RGUHSSep '25
DNBOct '24
DNBOct '24
MUHSWinter '24
RGUHSJun '24
DNBApr '23
DNBOct '23
DNBOct '23
MUHSWinter '23
MPMSUJun '23
DNBDec '22
DNBDec '22
DNBJun '22
RGUHSMay '22
RGUHSNov '22
RGUHSMay '22
RGUHSJul '21
DNBJun '21
DNBJun '21
DNBJun '21
MUHSSummer '21
MUHSWinter '21
MUHSWinter '21
RGUHSNov '21
RGUHSJul '21
RGUHSJun '20
MPMSU2020
DNBDec '20
DNBDec '20
DNBJun '20
MUHSSummer '20
MUHSSummer '20
MUHSWinter '20
RGUHSNov '19
RGUHSNov '19
RGUHSMay '19
RGUHSNov '19
RGUHSNov '19
RGUHSMay '19
MPMSUMay '18
RGUHSNov '18
MPMSUMay '18
RGUHSMay '18
RGUHSNov '17
MUHSSummer '17
RGUHSNov '17
MPMSUJun '17
MPMSUJun '17
RGUHSNov '16
RGUHSNov '16
RGUHSNov '16
DNBDec '16
DNBDec '16
MUHSSummer '16
MPMSU2016
DNBDec '15
MUHSWinter '15
DNBDec '14
DNBDec '14
DNBDec '14
DNBDec '14
DNBDec '14
DNBDec '14
MUHSSummer '14
MUHSWinter '14
MPMSU2014
DNBDec '13
DNBDec '12
DNBDec '12
DNBDec '12
MPMSU2012
RGUHSMay '11
DNBDec '11
DNBDec '11
MPMSU2011
MPMSU2011
RGUHSMay '11
RGUHSOct '10
RGUHSMay '10
RGUHSMay '10
RGUHSMay '10
RGUHSMay '10
MPMSU2010
RGUHSMay '10
RGUHSOct '09
RGUHSMay '09
MPMSU2009
MPMSU2009
RGUHSApr '08
MPMSU2008
MPMSU2008
RGUHSApr '07
RGUHSSep '07
MPMSU2007
RGUHSSep '06
RGUHSSep '06
RGUHSApr '06
RGUHSApr '06
MPMSU2005
MPMSU2002
Drug Dosage Principles & Individualisation
1. Definition, scope, and why dose individualisation matters
- Drug dose = the quantity of a drug administered per unit time to a given patient with the intent of producing a defined therapeutic effect while keeping the probability of toxicity acceptably low (G&G 14e Ch.2, pp.38–40).
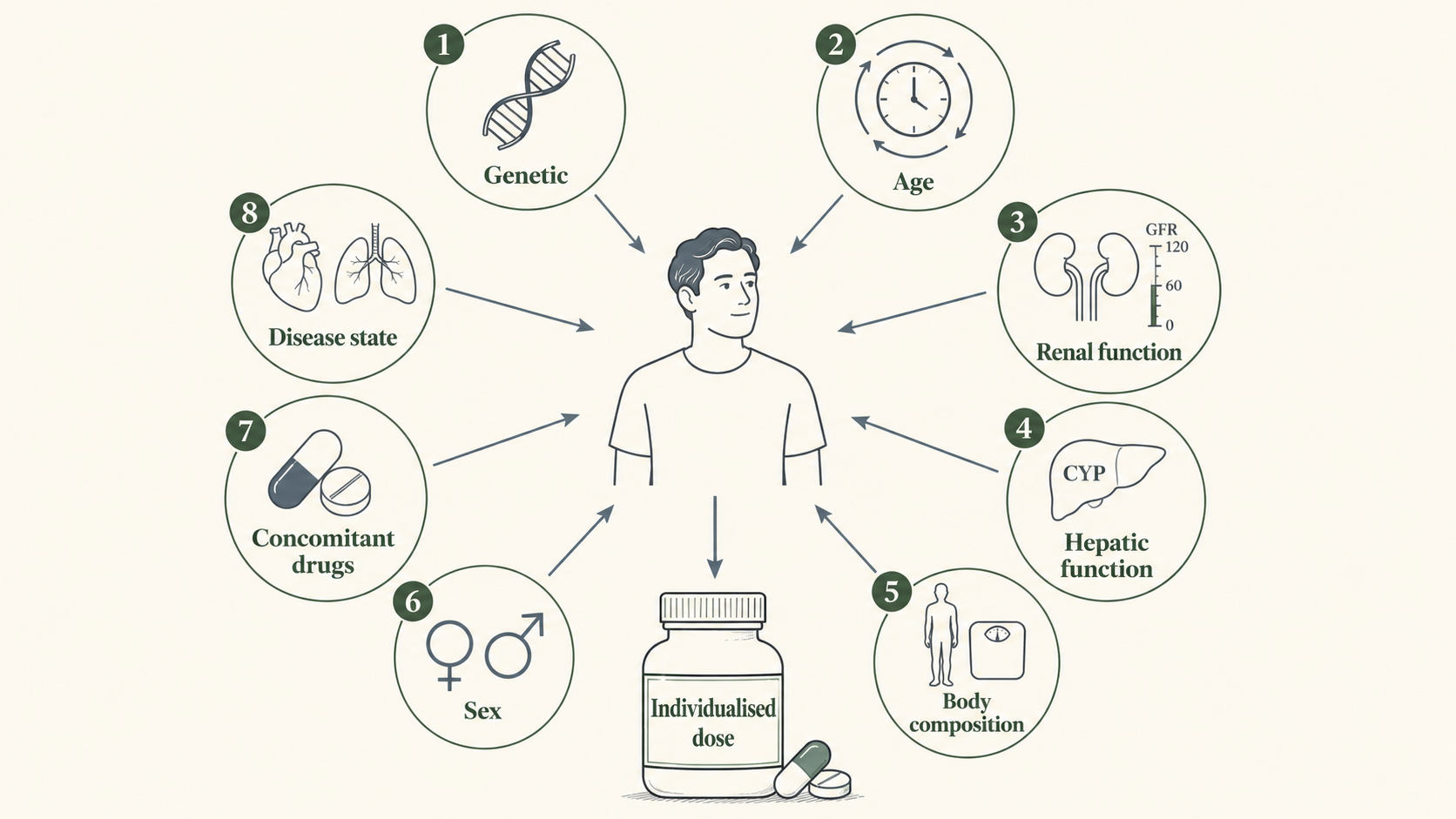
- Dose individualisation (synonyms: individualised dosing, personalised dosing, precision dosing) = the deliberate modification of a standard/labelled dose for a particular patient using patient-specific pharmacokinetic (PK), pharmacodynamic (PD), genetic, demographic, disease-state, and concomitant-therapy information so that the steady-state drug exposure lies within the therapeutic window (Shargel 8e Ch.21; Atkinson 4e Ch.2; R&T 2019 Ch.12).
- Why it matters — three drivers (G&G 14e Ch.2, p.39; B&B Ch.1):
- Therapeutic-window narrowness — for a small set of drugs (digoxin, theophylline, lidocaine, aminoglycosides, cyclosporine, tacrolimus, sirolimus, warfarin, lithium, phenytoin, valproate, carbamazepine, methotrexate) the upper limit of the therapeutic range is ≤2–3× the lower limit, so a labelled fixed dose will be sub-therapeutic in some patients and toxic in others.
- Inter-individual variability — apparent CL of a given drug can differ 5- to 30-fold between adults of similar weight and renal function because of genetic, environmental and disease-state factors (R&T 2019 Ch.12; Atkinson 4e Ch.9).
- Intra-individual variability — within the same patient, CL can shift over hours-to-days with disease progression, drug interactions, pregnancy, ageing, dialysis sessions, and concurrent illness (Atkinson 4e Ch.15; Shargel 8e Ch.23).
- The MD-level mandate (RGUHS PG syllabus, NMC competency PH 1.56) is to be able to (a) compute loading and maintenance doses from first principles, (b) modify them for renal, hepatic, pregnant, paediatric, geriatric and pharmacogenetically distinct patients, and (c) use plasma-concentration data to refine the regimen — i.e., to apply clinical pharmacokinetics at the bedside (Padmaja 7e Ch.63; KDT 8e Ch.5).
- Levels of individualisation (Atkinson 4e Ch.2; Shargel 8e Ch.21):
- Population-level — labelled dose derived from Phase 3 trials in a "typical" population.
- Sub-population–level — separate doses for paediatrics, geriatrics, renal/hepatic impairment, pregnancy (labelling supplements).
- Patient-level demographic — body weight, BSA, age, sex used in a formula.
- A priori PK — use of a population PK model with patient covariates to predict CL/Vd before any sample is drawn.
- A posteriori PK (Bayesian) — one or more measured plasma levels combined with a population prior to give a posterior estimate of CL/Vd for that patient → dose adjusted from this (the basis of modern TDM software, e.g. PrecisePK, DoseMe, InsightRx).
- Genotype-guided — a priori dosing based on CYP/transporter/HLA genotype (CPIC guidelines, FDA Table of Pharmacogenomic Biomarkers in Drug Labelling).
- Compliance with Indian regulatory framing — CDSCO requires labelling sections on use in renal/hepatic impairment, pregnancy and lactation, paediatric use, and geriatric use under Schedule Y of the New Drugs and Clinical Trials Rules 2019; these mirror FDA's PLLR-era expectations (KDT 8e Ch.5).
Continue reading
Drug Dosage Individualisation
PharmaNotes Pro · Comprehensive
Sign in with your Google account. If you're already subscribed, the chapter unlocks immediately — otherwise, pick Monthly or Annual on the next step.