Blinding, Randomization & Allocation Concealment in Clinical Trials
The three pillars of internal validity in randomized controlled trials
Past RGUHS + DNB + MPMSU + MUHS + VNSGU · 16
RGUHSSep '25
RGUHSMay '25
MPMSUJan '25
DNBDec '25
MUHSWinter '25
MPMSUJun '23
DNBOct '23
MPMSU2022
DNBDec '22
VNSGUApr '22
RGUHSNov '21
RGUHSNov '18
MPMSUJun '17
RGUHSMay '10
MPMSU2009
RGUHSSep '07
Blinding, Randomization & Allocation Concealment in Clinical Trials
1. Definition & overview — the three pillars of internal validity
- The randomized blinded trial (RCT), designed and conducted properly, provides the most definitive causal inference for evidence-based medicine and practice guidelines — it is the cornerstone of how cause and effect is proven and how a drug demonstrates the efficacy/safety needed to obtain a marketing licence (Browner 5e Ch.11; Bennett & Brown Ch.4).
- The two most important bias-avoidance techniques in trial design are randomisation and blinding; together they help avoid bias in the selection and allocation of subjects and in the measurement and assessment of outcomes (Bennett & Brown Ch.4).
- Randomization is the use of chance (probability) to assign treatments, so that no treatment assignment is known with certainty before the trial; it minimizes the influence of confounding variables — even those unknown or unmeasured — by distributing them equally (except for chance variation) across groups (Browner 5e Ch.11; MethodsCTStats Ch.68).
- Blinding (masking) prevents knowledge of the assigned treatment from biasing results; it minimizes differential placebo effects, differential cointerventions, and biased ascertainment/adjudication of outcomes (Browner 5e Ch.11; MethodsCTStats Ch.51).
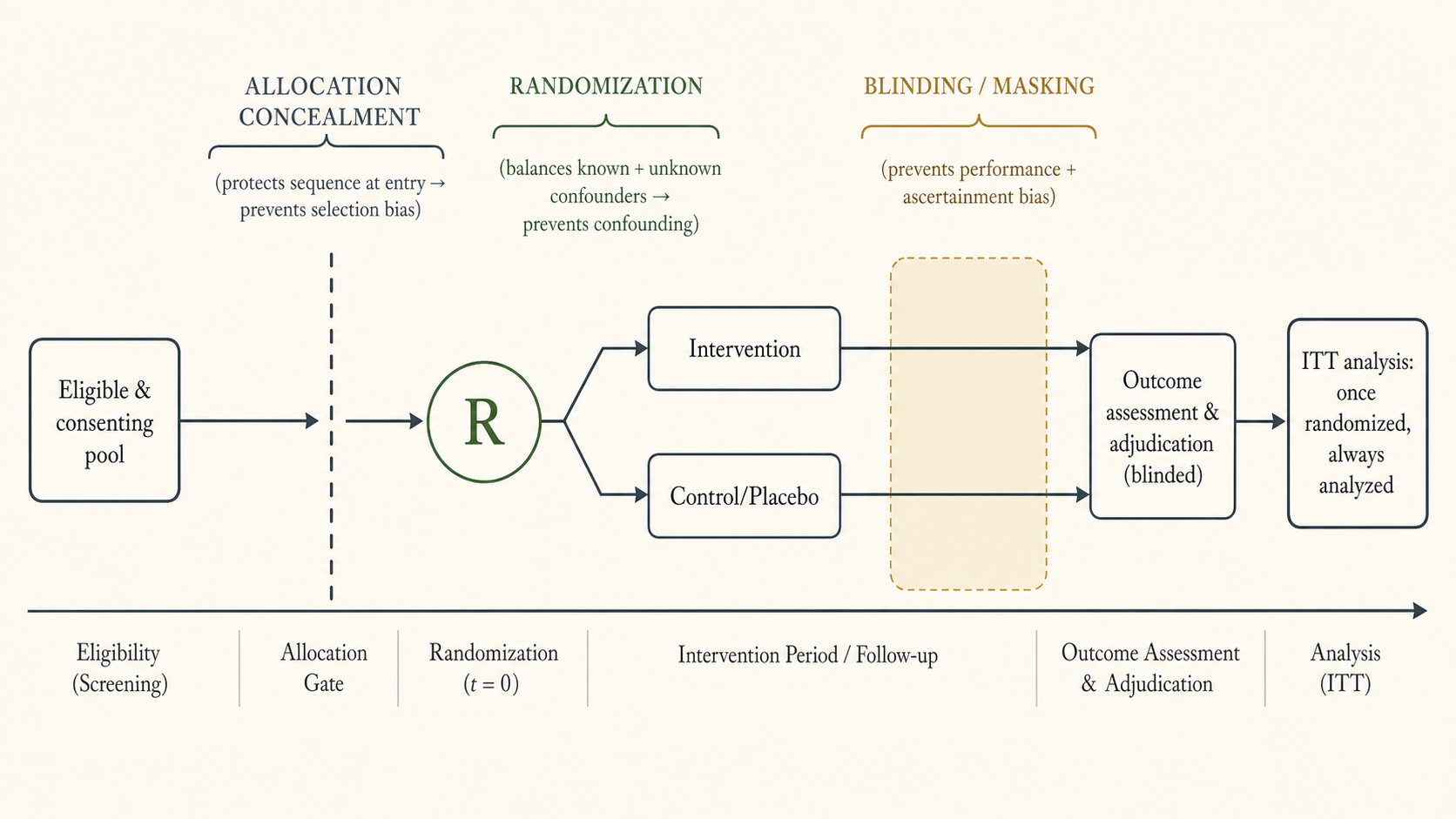
- Allocation concealment refers to whether the identity of the treatment for the next patient to be enrolled is known to those recruiting; it protects the integrity of the randomization sequence at the moment of enrolment and is distinct from blinding (MethodsCTStats Ch.51; Abramson Ch.32).
- Key conceptual separation (a high-yield exam point): allocation concealment operates before/at randomization (protects against selection bias in who gets enrolled into which arm); blinding operates after randomization (protects against performance bias, ascertainment bias, and differential cointervention/placebo effects during follow-up and outcome assessment) (MethodsCTStats Ch.51; Abramson Ch.32).
- The "classic" parallel-group RCT: select participants → measure baseline predictors (and baseline outcome level) → Randomly assign blinded intervention vs control (placebo or alternate drug) → follow over time minimizing loss to follow-up → measure outcomes; "parallel group" denotes intervention and control enrolled and followed concurrently (Browner 5e Ch.11).
- The ethical precondition for randomizing is equipoise (also "the uncertainty principle"): genuine uncertainty in the scientific community as to which arm is best, so that each participant has equal potential for benefit and risk (Bennett & Brown Ch.4; MethodsCTStats Ch.23, Ch.71; Abramson Ch.32).
Why each pillar matters (causal logic)
- Without randomization, treatments tend to be assigned by prognostic factors (e.g. severity), so sicker patients cluster in one arm — the experiment is confounded and treatment effects cannot be separated from underlying differences (MethodsCTStats Ch.68).
- Randomization provides the probabilistic basis for statistical inference: it guarantees the validity of statistical tests and lets one answer whether an observed difference is plausibly due to chance (MethodsCTStats Ch.71).
- An empirical, much-cited finding: across analyses of large numbers of trials, treatment effects are systematically smaller (closer to the truth) in trials that are double-blinded, and effects are exaggerated where allocation is poorly concealed — direct evidence that these are not optional niceties but bias-control essentials (Abramson Ch.32, citing the ~250-trial allocation-concealment analysis).
Continue reading
Blinding Randomization Allocation
PharmaNotes Pro · Comprehensive
Sign in with your Google account. If you're already subscribed, the chapter unlocks immediately — otherwise, pick Monthly or Annual on the next step.